





 |
CAH Community Action for Health Newsletter_2015 Dec |
|
|
1 Page 1 |
▲back to top |
Community Action for Health
Bringing Public into Public Health
Contents
01 Messages
03 Get-to-Know
04 Key Events
05 Updates
07 Case Stories
December 2015
Message from the National Health Mission
The National Health Mission
(NHM) lays particular emphasis
on the communitisation
process. An important component of
this process is Community Action for
Health which began as Community
Based Monitoring and Planning.
Community action is a key pillar of
NHM’s accountability framework.
The process enables communities
to actively participate and regularly
monitor the progress of the NHM
interventions in their areas and ensure
that health services are delivered
with quality, equity and prescribed
standards.
Community Action for Health
focuses on regular community
feedback to health service providers
and participatory local planning in
developing health plans and promoting
collective action to improve the delivery
of public health services. The Advisory
Group on Community Action (AGCA)
constituted by the Ministry of Health
& Family Welfare (MoHFW) in 2005
and comprising civil society experts,
advises the NHM on Community
action.
Beginning with a pilot implemented
between 2007-2009 which was
implemented in 9 states, Community
Action for Health is now being
implemented in 20 states and Union
Territories, with handholding support
from AGCA members and other
NGOs and funded through NHM. The
impetus now should be to strengthen
implementation of community action
process through existing structures. In
order to ensure sustainability and scale,
it is critical that states should now take
ownership of this process, by utilising
the human resources under NHM
and build capacity of Village Health
Sanitation & Nutrition Committees
(VHSNCs) at the community level and
Rogi Kalyan Samitis (RKSs) at the
facility level so that community action
for health is embedded in community
structures created under the NHM.
To enable sharing of best practices,
lessons learnt and replicable initiatives
across the country, the Ministry is
glad to launch the first edition of the
bi-annual newsletter developed by
AGCA the on Community Action for
Health. I seek your cooperation in
widely disseminating the newsletter
and applying the lessons to strengthen
implementation of community action
for health.
C K Mishra
Additional Secretary & Mission Director
Community Action for Health 01
|
|
2 Page 2 |
▲back to top |
Message from the Advisory Group on Community Action
Community action for health
ensures that people’s health
rights are met through a
process of active engagement by the
community in assessing the quality
and availability of entitled services.
The AGCA successfully led a pilot in
36 districts across nine states during
2007-2009, which demonstrated
positive outcomes of the community
action process towards improving
health services under the National
Rural Health Mission (NRHM).
An external review of the pilot
phase showed that strengthening
of the Village Health, Sanitation and
Nutrition Committees (VHSNCs)
provided a voice to the community,
especially the excluded and
marginalised groups. The process
resulted in an active engagement
between the community and the
health department, leading to an
increased knowledge on health
entitlements among the community
and improved service delivery. The
process also helped frontline health
workers to overcome service delivery
constraints through local planning
and community support.1
The AGCA, with support from the
MoHFW, is providing technical
assistance to the states to
strengthen and scale-up the
implementation of community
action for health. A team housed
in Population Foundation of India
as the AGCA Secretariat, supports
the states in facilitating state-level
visioning and planning exercises to
develop multi-year implementation
plans. The team facilitates capacity
building of state nodal officers and
implementing organizations. It also
provides support for adaptation of
manuals, tools and communication
materials, and undertakes periodic
implementation reviews.
We hope the newsletter will be
useful for State Health Secretaries,
NHM Mission Directors, State
Nodal Officers, training institutions
and officials from civil society
organisations to take forward and
strengthen the community action
process.
We invite you to share your
experiences and suggestions with us.
Poonam Muttreja
Advisory Group on Community Action
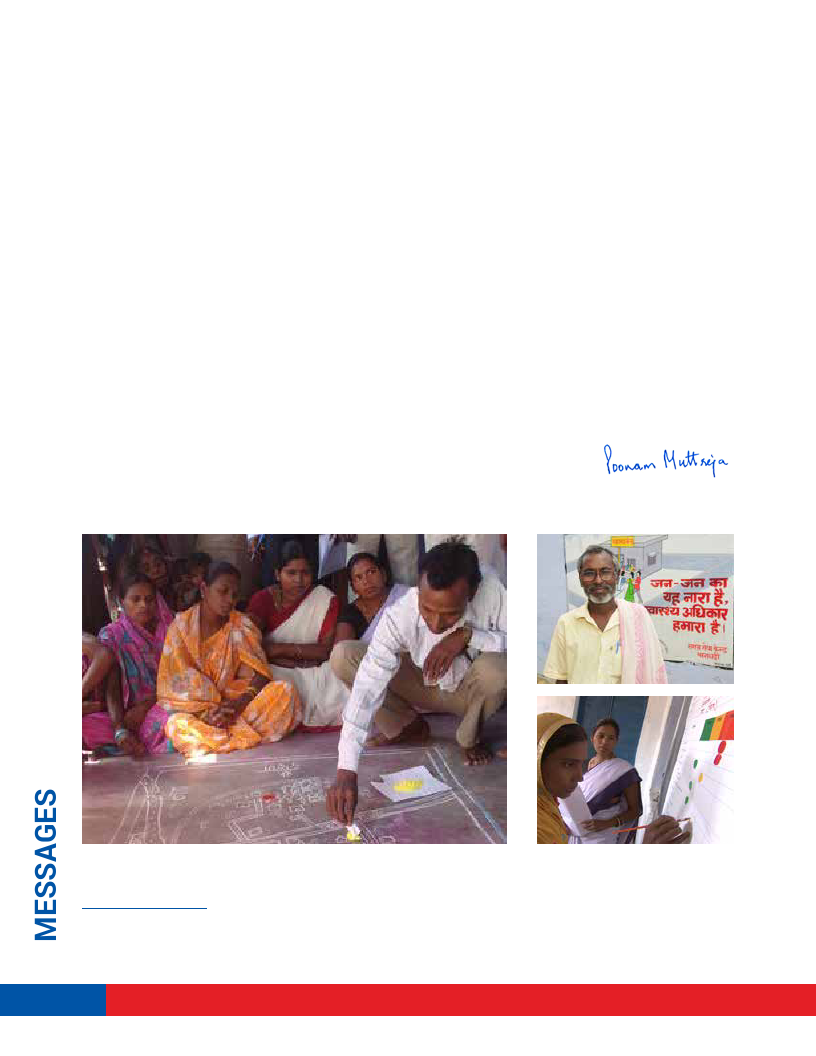
Activities under Community Action for Health - Village Health Mapping, a wall painting on health entitlements and developing a village health
report card.
1Reviving Hopes Realising Rights- A Report on the First Phase of Community Monitoring under the NRHM http://www.nrhmcommunityaction.org/
mediaupload/eva87287A_report_on_the_First_phase_of_Community_Monitoring.pdf.
02 Community Action for Health
|
|
3 Page 3 |
▲back to top |
What is Community
Action for Health?
Community Action for Health is
a key strategy of the National
Health Mission (NHM) which
ensures that the health needs and
rights of the community are being
fulfilled. It allows the people to
actively and regularly monitor the
progress of the NHM interventions
in their areas. Community Action
provides a mechanism to improve
accountability and enable better
delivery of services.
The Six Steps
Step 1. Creating Community
Awareness - on health
entitlements, health rights, roles
and responsibilities of service
providers.
Step 2. Strengthening Village
Health, Sanitation and Nutrition
Committees – Capacities of
VHSNCs are developed through
structured trainings and
mentoring.
Step 3. Formation and
Strengthening of Planning
and Monitoring Committees
(PMCs) – These committees are
formed at the Primary Health
Centre (PHC), block, district and
state levels to discuss and take
appropriate action on issues
emerging from community level
enquiries and facility surveys.
Step 4. Community Enquiries and
Facility Surveys - Health services
are monitored and evidence or
data collected through community
level enquiry and facility surveys
at sub-health centres and PHCs.
Step 5. Sharing of Report Cards
and Developing of Health Plans
Report cards are developed for
each health facility and village, and
services are categorised into Good,
Average and Poor. Thereafter,
discussions with service providers
are organised to identify steps to
improve the services.
Step 6 – Organising the Jan
Samwad (Public Dialogue) – The
cumulative village and facility
report cards and instances of
denial and poor quality of services
are shared by the community
with health officials during a Jan
Samwad. Plans are prepared along
with timelines and responsibilities
to redress the grievances and
gaps.
What does it lead to?
Enhanced trust and improved
interaction between the service
provider and the community
Improvement in service delivery
in ante natal and post natal
care services and immunization
coverage
Reduction in out-of-pocket
expenditure and demands for
informal payments
Active involvement of
Panchayat Raj members in
planning and monitoring the
functioning of health facilities
Participation of the most
excluded communities in the
village level monitoring and
planning processes
Appropriate planning and
utilisation of untied funds at
VHSNCs, PHCs, CHCs and RKS.
Where to seek guidance?
The AGCA provides guidance on
community action. The AGCA
comprises a group of 15 eminent
public health experts. The AGCA
Secretariat housed in Population
Foundation of India coordinates
the technical support to the
states, under the guidance of
AGCA members.
What are the essentials
for scaling up
community action for
health?
There is no ‘one’ prescriptive
model for scaling up community
action for health. Each state
has the flexibility to adapt and
contextualise the process as
per its context. Some of the
essentials to enable effective
scaling-up include -
Strengthening ASHA and
VHSNC support structures
and partnerships with credible
civil society organisations
Long-term support for building
capacities and confidence
of community institutions
to initiate and sustain the
community action process
Institutionalising
mechanisms for timely and
appropriate redressal of
grievances
Analysing issues and gaps
emerging from the community
action processes and
incorporating them into the
district and state PIPs.
Community Action for Health 03
|
|
4 Page 4 |
▲back to top |

National Consultation on Community Action for Health
The MoHFW and the AGCA jointly
organised a National Consultation
on Community Action for Health
on October 28 and 29, 2014 to
share experiences from community
action models and generate
recommendations to strengthen and
scale-up its implementation over the
next phase of the NHM.
The consultation brought together
123 participants from 25 states,
including senior government officials
from National and State Health
Missions, development partners, civil
society organisations, panchayat
representatives, the media and the
AGCA members. Keynote speakers
were Ms Aruna Roy (Mazdoor Kisan
Shakti Sangathan), who emphasized
on the community’s role in
governance and Mr Vinod Rai, former
Comptroller and Auditor General of
India, who appreciated the unique
partnership between the MoHFW and
Releasing key documents on Community Action for Health. (Left to Right) Ms Mirai
Chatterjee, Ms Poonam Muttreja, Dr Abhay Shukla (AGCA Members); Mr C K Mishra, Additional
Secretary and Mission Director (NHM), Ministry of Health and Family Welfare; Dr H Sudarshan,
AGCA Member; and Mr Vinod Rai, former Comptroller and Auditor General of India.
the civil society, while highlighting
the importance of accountability. Mr
C K Mishra, Additional Secretary and
Mission Director NHM, and Mr Manoj
Jhalani, Joint Secretary (Policy),
MoHFW reiterated the Ministry’s
commitment to a people-centered
health system. They emphasized
the need for states to adapt
and scale-up implementation of
community action for health.The
State NHM Mission Directors and
Nodal Officers shared the status
of implementation in the states,
challenges and commitments on
the way forward.
Launch of Community Action for Health in Mizoram
Mr Pu Lal Thanzara, Minister of
Health, Government of Mizoram,
launched the Community Action
for Health initiative in Aizawal on
February 6, 2014. Ms Esther Lal
Ruatkimi, Principal Secretary, Health
and Family Welfare, senior officials of
the health department, civil society
representatives and other
officials were present at the
event.
Mr Pu Lal Thanzara, Minister of Health, Government of
Mizoram, launching the Community Action for Health
programme.
Mr Pu Lal Thanzara
highlighted the importance of
increasing accountability of
health services to the people
as an important strategy for
health system strengthening.
He appreciated the ongoing
work by ASHAs, Village
Health, Sanitation and
Nutrition Committees
(VHSNCs) and Rogi Kalyan Samitis
(RKS) and urged all officials and
frontline health workers to provide
full support in implementing the
community action process.
The launch was followed by an
orientation workshop on the
community process for key state
government officials and civil society
representatives. Further, in-depth
discussions were held to pilot the
process in the state, beginning with
Serchhip district. Subsequently, the
AGCA supported the state in planning
the implementation of the pilot,
through the state NGO, Zoram Entu
Pawl.
04 Community Action for Health
|
|
5 Page 5 |
▲back to top |

Strengthening capacities
on Community Action
for Health
The AGCA provided technical
support to 25 states2 in the
financial year 2014-15 to plan
and roll-out the community action
process. The MoHFW approved the
budget for the component in 18
state Programme Implementation
Plans3.
State Advisory Group
on Community Action
State AGCAs have been formed to
provide guidance and oversight to
the community action process. The
AGCA provided support to 10 states
for constitution /reconstitution of
S-AGCA and oriented the members.
The S-AGCA meetings were
conducted under the chairmanship
of the Principal Secretary/Mission
Director in eight states: Uttar
Pradesh, Mizoram, Meghalaya,
Manipur, Odisha, Punjab, Rajasthan
and Karnataka. Efforts are underway
to constitute and strengthen the
committee in the remaining states.
The AGCA along with the S-AGCAs
is providing support to the states in
adapting the guidelines and manuals
to state specific context. The states
are also being supported to train the
master trainers on the community
action process.
Orientation Workshops
Orientation workshops on
Community Action for Health were
organized in eight states. This helped
Mr Hussan Lal, Mission Director, National Health Mission, Punjab shares the progress of the
community action for health programme in the state. (Left to right) Ms Sanghamitra Ghosh,
Mission Director, West Bengal; Mr P M Pradhan, Mission Director, Sikkim; Mr M R Synrem,
Mission Director, Meghalaya; and Mr Manoj Jhalani, Joint Secretary (Policy), MoHFW, who
chaired the session.
in developing a comprehensive
strategy to implement the
component:
In Odisha, a state-level Training
of Trainers was organised by the
S-AGCA in May 2014 with support
from the State NHM team.
Officials from the district health
department and other related line
departments such as Health &
Family Welfare, Women & Child
Development, Rural Development,
Panchayati Raj, School & Mass
Education, and the Scheduled
Caste & Scheduled Tribe
Development department were
trained as Master Trainers to
orient the NGOs and the District
Programme Management Units
(DPMU) on the Gaon Swasthya
Samikshya Programme, being
implemented in 52 blocks in
five districts through 49 NGO
partners.
In Uttar Pradesh, a workshop
was organised for the State
Nodal Officers in August
2014. Officials from the State
Programme Management Unit
(SPMU- Community Process),
State Innovation in Family
Planning Services Project Agency
(SIFPSA) and Technical Support
Unit participated. The state will
now implement the process in 36
blocks of 18 high priority districts.
In Meghalaya, an orientation was
held in August 2014 for the State
Community Processes team and
implementing partners. A detailed
implementation plans was
developed for three intervention
districts.
In Gujarat, an orientation was
organised for the State Nodal
Officer-Community Processes,
NGO representatives and other
stakeholders in August 2014.
2Arunachal Pradesh, Assam, Bihar, Delhi, Gujarat, Haryana, Himachal Pradesh, Jammu & Kashmir, Jharkhand, Karnataka, Kerala, Madhya Pradesh,
Maharashtra, Meghalaya, Mizoram, Nagaland, Odisha, Punjab, Rajasthan, Sikkim, Tamil Nadu, Tripura, Uttarakhand, Uttar Pradesh, West Bengal.
3Arunachal Pradesh, Assam, Chhattisgarh, Delhi, Goa, Gujarat, Jharkhand, Kerala, Madhya Pradesh, Maharashtra, Manipur, Meghalaya, Mizoram,
Odisha, Punjab, Rajasthan, Sikkim and Uttar Pradesh.
Community Action for Health 05
|
|
6 Page 6 |
▲back to top |

Dr Monica Rana, State Project Officer, Delhi interacting with MAS
members.
Mr Susant Nayak, Senior Consultant, Community Processes, Odisha
facilitating a session at an orientation workshop.
The process will be scaled-up in
77 blocks, across the eight high
priority districts.
In Mizoram, the AGCA Secretariat
and SATHI facilitated a two-day
consultation on community
processes in December 2014.
The members of the ASHA
Resource Centre and the State
Mentoring Group, state-level
programme heads and other
stakeholders participated.
In Delhi, the Community Action
for Health process is being
initiated in selected wards/
mohallas in eight districts
covering 100 Mahila Arogya
Samities (MAS). The state and
district level NHM officials were
oriented in April 2014. Meetings
were held with the New Delhi
Municipal Corporation and the
Delhi State Health Society to
chalk out the implementation
plan.
status of community action
in two blocks of Ranchi
district in December 2014. A
meeting was also held with
the State Sahiya Mentoring
Group and suggestions were
made to strengthen the group
by including members from
the civil society and line
departments.
Resource materials
Guidelines and Manuals
The Guidelines for Programme
Managers and the User Manual
on Community Action for Health
have been developed to guide
implementing organizations and
health managers to effectively roll-
out community action processes at
the state, district and block levels.
Monograph on Community Action for
Health
The monograph captures the
experiences, challenges and lessons
learnt from the community action
processes across India and South
East Asia. The document includes
detailed case studies of five
programmes/projects across India.
A Documentary Film
The film, Bringing Public into Public
Health captures experiences from
different models and processes of
community action for health across
the country, which have yielded
positive results and contributed to
improved delivery of health services.
The film is part of the training kit.
The resource materials can be
accessed on the AGCA website –
www.nrhmcommunityaction.org .
In Punjab, the AGCA oriented
members on the community
action process and supported
in developing plans for visioning
and planning workshops in the 11
scale-up districts.
In Jharkhand, the AGCA team
reviewed the implementation
06 Community Action for Health
|
|
7 Page 7 |
▲back to top |
Leveraging the State Institute of Rural Development for VHSNC trainings
The State NHM, Punjab has developed a unique partnership with the State Institute of Rural
Development (SIRD) to train VHSNCs across 20 districts. To initiate the process, the AGCA trained a
pool of 30 state-level Master Trainers, including SIRD faculty members in 2012.
A total of 160 Master Trainers and 75,708 VHSNCs members were trained during 2012-14 in two
phases by the SIRD faculty and health experts from the State Health Society. The process was rolled
out in coordination with the Additional District Collector and Block Development and Programme
Officers (BDPOs). Forty three teams comprising three Master Trainers each, facilitated a two-day
training for the VHSNC members at the panchayat /village level. SIRD deputed a supervisor to
monitor the quality and content of the training. VHSNC trainings will now be initiated in 11 new
districts.
Positive outcomes of engagement with SIRD
Over 90% Panchayati Raj Institution (PRI) members participated in the training.
Community Action for Health has been included in the regular curriculum for training of PRI
members, Rural Development officials and in induction of BDPOs.
A specific training on Community Action for Health has been initiated for District Programme
Managers, Deputy Chief Medical Officers and Medical Officers In-charge.
SIRD has included questions on community action in the gram panchayat evaluation under the
Panchayat Sashaktikaran Puraskar initiative.
Glimpses of positive outcomes
from Community Action
Meghalaya began implementing the
community action process in 2011, with
facilitation support from civil society
organisations. The efforts have shown
promising results. People of Kasinda
village access health services from the
Primary Health Centre located in block
Shella, East Khasi Hills district. The
centre would earlier refuse to issue birth
certificates for newborns. The community,
empowered through the community action
process, raised the issue with the Deputy
Commissioner, who took prompt action. The
PHC is now issuing birth certificates.
Community Action for Health 07
|
|
8 Page 8 |
▲back to top |

Grievance redressal: An example from Melghat, Maharashtra
The community monitoring programme is being implemented in Maharashtra since 2007. There is
now the realization that with increased awareness on rights, there is a need for a grievance redressal
mechanism to look into and resolve public grievances. Thus, over the last one year, block and district
level Grievance Redressal Committees have been set up in selected districts.The Takrar Nivaran Samiti or
Grievance Redressal Committee in Dharani block, a tribal dominated area in Amravati district, is one such
committee. The Takrar Nivaran Samiti has the Taluk Health Officer, the Medical Superintendent of the Sub-
district Hospital, a representative from the ICDS programme, the Sabhapati of the Panchayat Samiti, and
representatives from both civil society and the media as its members. The committee meets once every
quarter to discuss and address grievances. The committee receives grievances from both the community
and health care providers and also takes cognizance of issues arising from the community monitoring
process.
When a pregnant woman attending the sub-district hospital was found to have a very low haemoglobin
level, the doctors referred her to the Amravati District Hospital, about four hours away. However, the woman
and her husband refused to go as they said there was no one to take care of their children at home. The
doctors sought help from the committee members. The members convinced the couple to go to the district
hospital and simultaneously made arrangements for the care of the children. To ensure the woman received
adequate care, one of the members regularly followed up with the Civil Surgeon at the District Hospital. This
highlights how a grievance redressal committee can foster community action much beyond just redressal
of grievances, and can ensure better health outcomes.
AGCA members
Mr A R Nanda
Former Executive Director
Population Foundation of India
Dr Abhay Shukla
Co-ordinator
SATHI- CEHAT
Dr Abhijit Das
Director
Centre for Health and Social Justice
Mr Alok Mukhopadhyay
Chief Executive Officer
Voluntary Health Association of India
Mr Gopi Gopalakrishnan
President
World Health Partners
Dr H Sudarshan
Honorary Secretary
Karuna Trust
Dr Vijay Aruldas
Ex-General Secretary
Christian Medical Association of India
Ms Indu Capoor
Founder Director and Director
CHETNA Outreach
Ms Mirai Chatterjee
Director
SEWA Social Security
Dr Narendra Gupta
Coordinator
PRAYAS
Dr M Prakasamma
Director
Academy of Nursing Studies
Dr Saraswati Swain
Secretary General, NIAHRD
Dr Sharad Iyengar
Chief Executive, ARTH
Dr Thelma Narayan
Director
Community Health Cell, SOCHARA
Ms Poonam Muttreja
Executive Director
Population Foundation of India
Advisory Group on Community Action
Secretariat
Population Foundation of India
B-28, Qutab Institutional Area, New Delhi-110016
Tel: 011-43894100; Fax: 011-43894199
Email: agca@populationfoundation.in
www.nrhmcommunityaction.org
08 Community Action for Health