





 |
Issue Briefs - Sex Seletion in India |
|
|
1 Page 1 |
▲back to top |

parties are gainers in this matter...The parents are able
to get rid of the foetus of the unwanted sex and the
service providers benefit financially. Neither of these two
parties would be complainants.”5 The Ministry points
to the resulting non-availability of evidence as a major
hindrance in identifying cases of female foeticide.
Government Schemes
State governments have implemented certain schemes to
encourage families to have girl children. For example,
Tamil Nadu enacted a Cradle Baby Scheme in 1992.
There have been mixed reports on the program, including
reports that said many of the ‘cradle’ babies died.3 There
has been no cradle baby in recent years.14 Tamil Nadu
also initiated a Rs 35-crore Girl Child Protection Scheme,
which gives money to families who undergo family
planning operations after having one or two girl children.15
Haryana recently announced the implementation of a
Ladli Scheme, in which the government provides families
who have a second girl child with Rs 5,000 per year for
five years. On March 8, 2008, the Delhi government
also launched a Ladli Scheme, in which, “The Delhi
Government would deposit Rs 10,000 in the name of
a girl child at the time of her birth and subsequently an
amount of Rs 5,000 each would be deposited at the time
of her admission to Class I, VI, IX, X and XII. Finally, an
accumulated amount of about Rs 1 lakh would be made
available to every girl child on their attaining the age of 18
years provided they had passed at least Class X.”16
The centrally-sponsored Balika Samriddhi Yojana
provides a post-birth grant of Rs 500 for girl children
born on or after August 15th, 1997 and provides
scholarships from Rs 300 to Rs 1,000 for each
successfully completed year of schooling.17 Additionally,
the Central Government announced on February 19,
2007 that it is enacting a new scheme, to be implemented
by the Ministry of Women and Child Development in
coordination with state governments as part of the 11th
Plan. Under this scheme, palnas, or cradles, would be
kept in every district for families to drop off unwanted
girl children to prevent further female foeticide.18
Endnotes
1. Guilmoto, Christophe Z., “Characteristics of Sex-Ratio Imbalance in India,
and Future Scenarios,” UNFPA, October, 2007. See http://www.unfpa.
org/gender/docs/studies/india.pdf.
2. NFHS1998/99. Note: Post-neonatal mortality, or the probability of death
between one month and one year of age was higher for females (26.6) than males
(24.2).
3. Krishnakumar, Asha, “Scanning for Death,” Frontline, Volume 15: No. 25:
Dec 5-18, 1998.
4. Census, 2001.
5. Ministry of Health and Family Welfare, PNTD Division Annual Report on
implementation of the Pre-Conception and Pre-Natal Diagnostic Techniques
(Prohibition of Sex Selection) Act, 2005.
6. Sabu George, “Letter: Sex Ratio in India,” Lancet. In a response to Jha, P,
Kumar R, Vasa P, Dhingra N, Thiruchelvan D, Moineddin R. Low male-
to-female sex ratio of children born in India: national survey of 1.1 million
households. Lancet 2006; 367: 211-18). Dr. George challenges both the data
set and the methodology the researchers used.
7. Sabu George. See http://www.hsph.harvard.edu/grhf-asia/forums/foeticide/
articles/foeticide.html.
8. Madhu Gurung, “Demographic danger signals,” Frontline, Volume 17, Issue
02, Jan. 22- Feb. 4, 2000.
9. Zaidi, Annie, “For a legal deterrent,” Frontline, Volume 22, Issue 20,
Sep. 24- Oct 7, 2005. See http://www.hinduonnet.com/fline/fl2220/
stories/20051007002704600.htm.
10. See http://mohfw.nic.in/dofw%20website/acts%20&%20rules/Ju dgment_
Palwal.htm. See also “Social activist thrilled at conviction,” Hindu, April 2,
2006,http://www.hindu.com/2006/04/02/stories/2006040209400400.
htm.
11. Office Memorandum No. 24026/III/06-PNTD Ministry of Health and
Family Welfare, Feb 12, 2007.
12. Duin, Julia “GE Machines Used to Break Laws,” Washington Times, March
1, 2007.
13. The London Daily Mail reported 70,000 and the British Medical Journal
estimated about 100,000 ultrasound machines. Cited by Julia Duin (see note
12).
14. “Scanning centres warned against female foeticide,” The Hindu, September 11,
2004.
15. “Over 1,000 children rescued under Cradle Baby Scheme,” The Hindu,
November 16, 2004.
16. “Newborn Prachi becomes first ‘Ladli,’” The Hindu, March 8, 2008. See
http://www.hindu.com/2008/03/08/stories/2008030853610400.htm.
17. Guidelines for the Balika Samriddhi Yojana. See http://wcd.nic.in/BSY.
htm.
18. “Government set to ‘cradle’ girl child,” Times of India, February 19, 2007.
DISCLAIMER: This document is being furnished to you for your information. You may choose to reproduce or redistribute this report for non-commercial
purposes in part or in full to any other person with due acknowledgement of PFI and PRS Legislative Research (“PRS”). The opinions expressed herein are
entirely those of the author(s). PRS makes every effort to use reliable and comprehensive information, but PRS does not represent that the contents of the
report are accurate or complete. PRS is an independent, not-for-profit group. This document has been prepared without regard to the objectives or opinions
of those who may receive it.
Population Foundation of India
B-28, Qutab Institutional Area, New Delhi-110016
Tel.:+91-11-43894100, Fax: +91-11-43894199,
E-mail: popfound@sify.com, Website: www.popfound.org
Sex Selection in India
Issue Brief
Context
• Sex Selection refers to the practice of determining the sex of the foetus and eliminating
it if it is female.
Child Sex Ratios
(CSR) and Overall
Sex Ratios (OSR)
1951-2001
Year CSR OSR
1961 976 941
1971 964 930
1981 962 934
1991 945 927
2001 927 933
Source: 2001 Census, “Sex
Composition of the
Population” Chapter 6.
• India has one of the lowest Overall Sex Ratios in the world (933 females per 1000
males), falling behind neighbours Pakistan, Bangladesh and China. Moreover, a
significant decline has been observed in India in the Child Sex Ratio of children aged
0-6 from 945 girls per 1,000 males in 1991 to 927 girls per 1,000 boys in 2001.
• Over 80% of districts in India recorded a drop in the Child Sex Ratio between 1991
and 2001. This sudden drop is believed to be a result of the growing practice of sex
selection and prebirth elimination of females.
Government Initiatives
• The Pre-conception and Pre-natal Diagnostic Techniques (Prohibition of Sex Selection)
Act 1994 (PCPNDT Act) prohibits use of technology, such as amniocentesis and
ultrasound techniques, for sex selection in order to eliminate the foetus based on sex.
The first conviction was obtained only in January, 2006.
• Government Schemes to encourage parents to have girl children vary from state to state.
Tamil Nadu enacted a Cradle Baby Scheme in 1992, as well as a Girl Child Protection
Scheme. Haryana and Delhi’s Ladli Schemes give financial incentives to families with
daughters.
• The centrally-sponsored Balika Samriddhi Yojana provides a post-birth grant of Rs
500 for girl children born after August 15, 1997 as well as annual scholarships for each
successful year of schooling.
• In 2007, the Central Government announced a scheme in which palnas, or cradles, will
be put in every district for families to drop off unwanted girl children.
Prepared by
PRS Legislative Research, Centre for Policy Research, Dharma Marg, Chanakyapuri, New Delhi – 110021
Tel: (011) 2611 5273-76, Fax: 2687 2746, www.prsindia.org
|
|
2 Page 2 |
▲back to top |
The Issue
The Child Sex Ratio (CSR) is the number of girls in the
age group of zero to six years per thousand boys of
the same age group. According to the 2001 Census, the
CSR declined from 945 females per 1000 males in 1991
to 927 females per thousand males in 2001. According
to the United Nations Population Fund (UNFPA), “Sex
selection appears to have played a major role in causing
the deterioration observed in child sex ratio. Excess
female mortality among infants and children contributes
only moderately to the deficit of girls.”1 In fact, neonatal
morality (death within one month of birth) is higher for
boys (50.7) than girls (44.6)2 While the child sex ratio
has decreased since 1961, there has been a more rapid
decrease since 1981.1
While the practice of female infanticide (killing the
girl child post-birth) has been reported earlier in
India, female foeticide has arisen recently following
technological developments over the last 30 years.3 The
reason for this dramatic shift relates to the introduction
into India of methods of prenatal sex determination,
such as amniocentesis and ultrasound technology.1
These technologies, intended to improve mother and
child health, had “the unexpected option of offering
couples advanced information on the sex of their future
children.”
Some reasons this method seems to be preferred and
used more include: (a) its high level of efficiency in
terms of outcome, (b) services are provided by medical
practitioners and considered ‘safer’, (c) a shortened
process, and (d) an easier method to conceal early
pregnancies from the community.1 India’s Overall Sex
Ratio is already one of the lowest in the world, falling
below neighbours Bangladesh, Pakistan, and China.
Trends
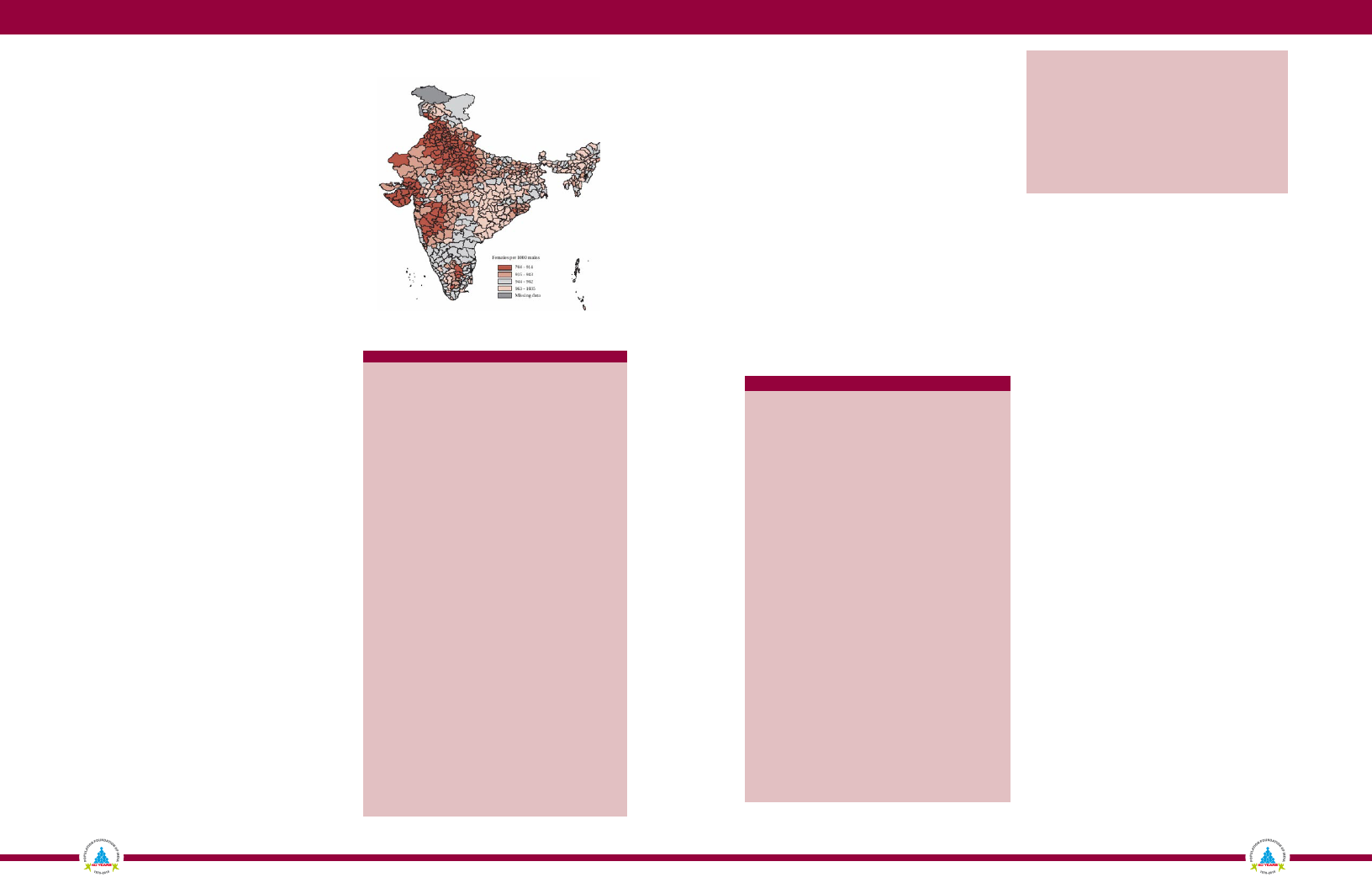
The worsening of the child sex ratio has been observed
particularly in the west and northwest of the country,
stretching from Punjab to Maharashtra. As of
2001, Punjab (793:1000 males), Haryana (820:1000),
Chandigarh (845:1000), Delhi (865:1000) and Gujarat
(878:1000) are the states with the lowest CSR. Between
1991 and 2001, more than 80% of districts in India
recorded a drop in the child sex ratio.4
While CSR is lowest in the north-western and western
states, even “better performing” states such as Tamil
Nadu, Madhya Pradesh and Orissa have a few districts
with CSR significantly below the national average.4
Figure 1: Child Sex Ratio in Districts of India,
2001
Source: Census 2001, Office of the Registrar General and Census Commissioner,
Ministry of Home Affairs, 2001
Table 1: State-wise CSRs between 1991-2001
1991
INDIA
945
Punjab
875
Haryana
879
Chandigarh
899
Delhi
915
Gujarat
928
Himachal Pradesh
951
Uttarakhand
948
Rajasthan
916
Uttar Pradesh
927
Maharashtra
946
Daman & Diu
958
Madhya Pradesh
941
Goa
964
Jammu & Kashmir
NA
Bihar
953
Tamil Nadu
948
Karnataka
960
Orissa
967
Pondicherry
963
Manipur
974
Arunachal Pradesh
982
Kerala
958
West Bengal
967
Andhra Pradesh
975
Assam
975
Andaman & Nicobar
973
Jharkhand
979
Mizoram
969
Dadra & Nagar Haveli
1013
Lakshadweep
941
Tripura
967
Chhattisgarh
984
Meghalaya
986
Nagaland
993
Sikkim
965
2001Change
927
-18
793
-82
820
-59
845
-54
865
-50
878
-50
897
-54
906
-42
909
-7
916
-11
917
-29
925
-33
929
-12
933
-31
937NA
938
-15
939
-9
949
-11
950
-17
958
-5
961
-13
961
-21
963
+5
963
-4
964
-11
964
-11
965
-8
966
-13
971
+2
973
-40
974
+33
975
+8
975
-9
975
-11
975
-18
986
+21
Source: 2001 Census. Lower figure indicates fewer girls in population.
According to the 2001 Census, some religious groups,
such as Sikhs or Jains, exhibit worse sex-ratio values on
the whole, while CSR tends to be normal or low among
other groups, such as tribal communities.1
Factors Leading to Sex Selective Abortion
According to the Ministry of Health and Family Welfare,
the causes for the elimination of the girl child are rooted
in rituals and perceptions such as dowry, beliefs that sons
must perform the last rites, male lineage and inheritance,
and social and economic security.5 Studies show that
preference for a male child and demand for pre-natal
sex determination techniques drastically increases for
the second child, when the first child is a girl.6
Related Legislation
Amniocentesis, a pre-natal technology, started in India
in 1974 as a part of a sample survey conducted at the
All India Institute of Medical Sciences to detect foetal
abnormalities. The first sex determination clinic opened
in Amritsar in 1979.7,8
Table 2: Timeline of Key Legislation
Year Legislation
Purpose
1956 Indian Medical CouncilDoctors are legally bound to report medical
Act, 1956
malpractice.
1971 Medical Termination ofLegalized abortion for health-related reasons.
Pregnancy Act, 1971
1988 MaharashtraThe first state law enacted in Maharashtra
Regulation of Use of against sex determination.
Prenatal Diagnostic
Techniques Act, 1988
1994 Pre-conception and
Pre-natal Diagnostic
Techniques Act and
Rules (PCPNDT),
1994
Mandates that sex selection by any person,
by any means, before or after conception, is
prohibited. Three-year imprisonment and
Rs10,000 fine.
Jan Supreme Court Order Directed state governments to enforce PNDT
26,
and file an affidavit indicating the status of
2002
action taken under the Act.
Directed five multinational companies to
give names and addresses of the clinics
and persons in India to whom they had sold
machines in past five years.
2002 Amendment of theEstablishes guidelines as to where and by
Medical Termination of whom medical terminations of pregnancies
Pregnancy Act
may be carried out, and specifies
imprisonment for violators.
2003 Amendment to
PCPNDT
Provides explicit provisions for the use,
regulation and monitoring of ultrasound
machines to curb their misuse for detection
of the sex of the feotus.
Pre-conception introduced.
Prescribes imprisonment up to five years
and a fine up to Rs.1,00,000.
Source: PRS.
The PCPNDT Act 1994
• Regulates prenatal diagnostic techniques (e.g. amniocentesis and
ultrasonography) for detection of genetic abnormalities, by restricting
their use to registered institutions, for a specified purpose and by a
registered person.
• Prevents misuse of such techniques for sex selection before or after
conception.
• Prohibits advertisement of any technique for sex selection as well as
sex determination.
• Prohibits sale of ultrasound machines to persons not registered under
this Act.
Implementation of PCPNDT Act
The biggest challenge with the Legislation seems to be
at the implementation stage. Since the implementation
of the Act until October 2005, 300 cases have been
registered under the PNDT Act, of which 214 relate
to non-registration, 10 relate to non-maintenance of
records, and 24 cases are about communicating the sex
of the foetus.9 Since its notification in 1994, the first
conviction was obtained only in January 2006.10
The Act establishes a Central Supervisory Board (CSB)
under the Chairmanship of the Union Minister for Health
and Family Welfare to monitor its implementation.
Parallel boards exist in each state and union territory
and are required to submit quarterly reports to the
Ministry. In 2005, six states did not submit reports, the
CSB did not meet in fifteen states, and no inspections
were conducted in at least five states. However, reporting
states had each conducted awareness campaigns.5
Until February 2007, the Chief Medical Officer (CMO)
served as the Appropriate Authority to monitor the
implementation of the Act. On February 12, 2007,
the CSB appointed the District Magistrate (DM) as the
Appropriate Authority instead. They have the power
of a Civil Court for search, seizure and sealing of the
machines, equipment and records of the violators.11
The law may be difficult to implement because the same
technology used for sex determination and selection
is legal for detection of genetic abnormalities in the
foetus. It may be difficult to monitor whether couples
are using the technology for legal purposes. Currently
25,770 ultrasound machines are officially registered with
the government.12 According to some reports, there
may be anywhere from 70,000 to 100,000 machines in
the country.13 In Punjab alone, there are estimated to be
1,000 to 1,500 ultrasound clinics.7
Medical practitioners also play an important role in
the implementation of the law. It is their responsibility
to refuse conducting sex determination, as well as
to maintain proper records of the use of pre-natal
technology. However, “Unlike in other cases, both