





 |
PFI Policy Brief - Planned Families |
|
|
1 Page 1 |
▲back to top |
Population Foundation of India
Policy Brief/2013
Planned Families in India:
A national development approach
Family planning is a critical element of reproductive health,
economic development and women’s empowerment.
Improving Health Outcomes
India’s Total Fertility Rate (TFR)
has declined from 5.2 in 1971 to
2.5 in 2010.1 This overall decline
suggests an improvement in
both access to contraceptives
as well as in the control that
Indian women have been able to
exercise over their reproductive
lives. However, there is still a
very long way to go. Estimates
from 2005-06 show that 13% of
pregnancies still occur among
women aged 18 or below and
only 5% of married adolescents
under 18 report any use of
modern
contraceptives.2
Studies also document that
21% of pregnancies in India
are unplanned.3 Such births
negatively affect maternal and
child health and survival in
many ways.
Evidence shows that family
planning directly reduces the
number of maternal deaths
because it lowers the risk of
unplanned pregnancy and
its associated complications,
lowers the risk of having an
unsafe abortion, delays first
pregnancy in young women who
might have premature pelvic
development and reduces risks
for women whose health may
already be compromised.
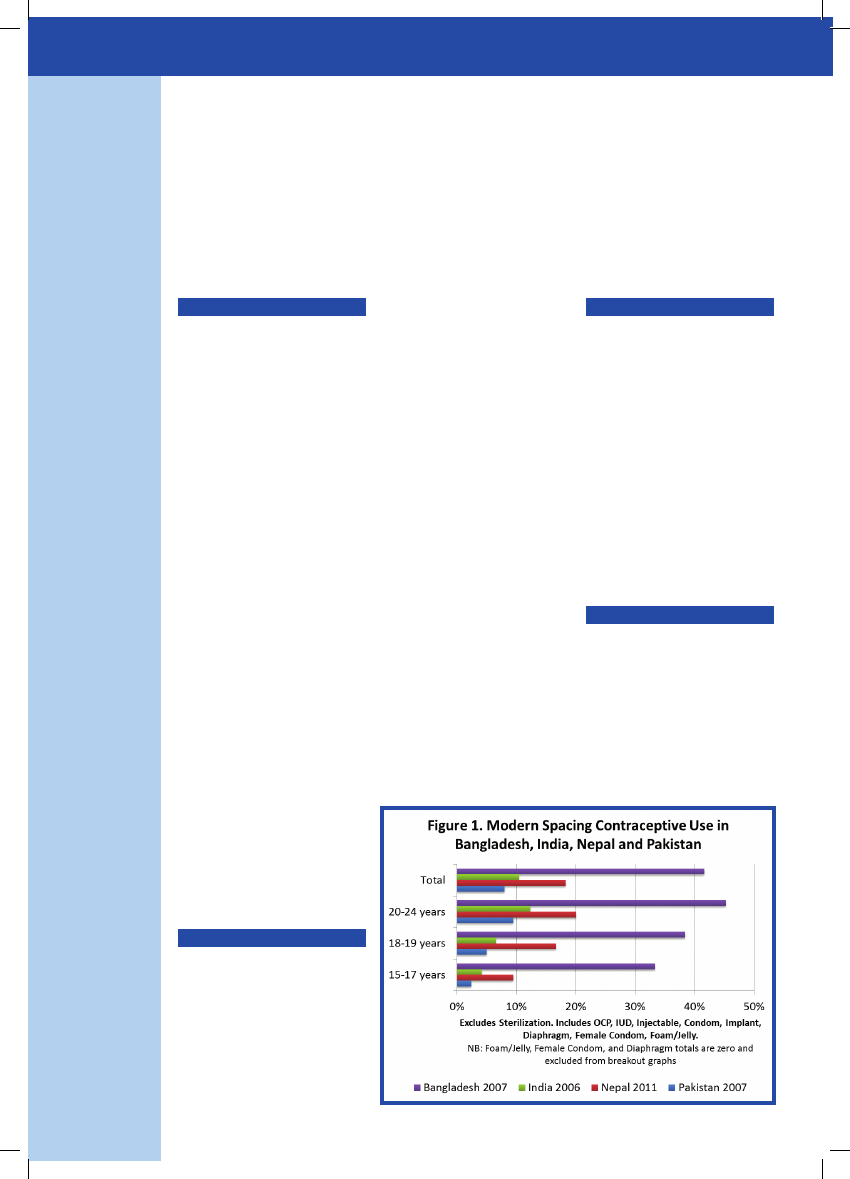
mortality.4 The persistent
unmet need for family planning
has contributed to “inadequate
progress” towards reducing
maternal mortality in India and
as can be seen in Figure 1 below,
use of spacing methods of
contraception are significantly
higher in Bangladesh than
India.
Globally, if voluntary family
planning is used to its fullest
potential and all unmet need,
met, then contraceptive use
can avert well over half of all
maternal deaths. This finding
has profound implications for
policies on maternal health and
child survival and emphasises
the urgency of meeting the
contraceptive needs of an
estimated 32 million women
in India whose needs are
still unmet.6 Family planning
therefore is a key intervention
to prevent maternal mortality.
Improving Child Health
Delaying age at marriage,
improving quality of care of
family planning services and
contraceptive use improves
child survival by ensuring
appropriate timing of births
(when a woman is physically
and mentally prepared to bear
a healthy child) and lengthening
birth intervals. Access to
family planning can reduce
infant mortality by 10% and
childhood mortality by 21%.7
Family planning therefore, is a
key investment in the health of
women and children.
Improving Economic Outcomes
Beyond health, there are
many far-reaching, catalytic
effects of family planning. At
the household level, families
are able to invest more of
their scarce resources in the
education of their children.
In India contraceptive use is estimated to have averted between
85-90,000 deaths in 2008.10
Averting Maternal Death
India continues to account for
one fifth of all maternal deaths
globally. Where neighbouring
Nepal and Bangladesh have
both achieved or are on target
to achieve MDG 5A - reducing
maternal deaths by 75% by 2015,
India continues to stagnate with
only a 50% reduction in maternal
|
|
2 Page 2 |
▲back to top |

Policy Brief/2013
Population Foundation of India
Universal & Comprehensive Family
Planning can transform a woman's
life by:
1. Delaying the age of first
pregnancy, giving her the
opportunity to complete her
education and enter the workforce.
2. Spacing children which
improves both maternal and child
health, and her ability to work
outside the home or acquire new
skills.
3. Providing access to pro-
women contraceptive options,
empowering her to plan her family.
Girls from smaller families are
more likely to complete their
education. Access to family
planning is likely to have an
economic impact for families.
Fewer children enable women
to seek employment, thereby
increasing household income
and assets. Therefore, parents
can invest more money and time
per child in health, nutrition
and education. These early
childhood investments can
have large effects on physical
and cognitive development
and education outcomes
and subsequently, income in
adulthood. Investments also
increase prospects for the next
generation, alleviating poverty
by boosting labour productivity
and capital accumulation which
leads to economic growth.
Family Planning would therefore
enhance the capacity of our
government to improve human
capital, reduce poverty and
hunger and enable communities
to maximize their use of natural
resources and adapt to the
consequences of climate
change and environmental
degradation.
Family planning therefore, is a key investment in
the health of women and children.
Millions of girls and women
can transform their lives if
their needs for voluntary and
comprehensive family planning
- to delay, space and plan the
number of children they have -
are met .
Family planning is recognized
as a highly cost-effective
development intervention
to promote healthy families,
increase opportunities for
economic development and
enable a strong and vibrant
nation. The UN recognizes
that “for every US dollar spent
in family planning, between
US$2 and US$6 can be saved
in interventions aimed at
achieving other development
goals.”8 Family planning,
therefore is a key investment
as it helps reduce the costs of
healthcare.
Falling birth rates also have the
potential for a ‘demographic
dividend’ by increasing the
economic and health returns on
investments in family planning,
it is imperative to remember
that family planning is above
all a matter of the individual’s
human rights.
The right to contraceptive
information and services are
inalterably linked to the principle
of non-discrimination and the
rights to health, information
and education, privacy and
life.10 Each of these human
rights are connected to the
other. For instance, the right to
the highest attainable standard
of health, which includes access
to health services and health
related information, cannot be
fulfilled without the protection
and promotion of the right to
education and information.
The human rights principle
requires that contraceptive
information and services are
available and accessible to all
groups.11 Refugees, internally
Millions of girls and women can transform their
lives if their needs for voluntary and comprehen-
sive family planning - to delay, space and plan the
number of children they have - are met.
ratio of working adults to
dependents. This rise leads to
a higher proportion of people in
paid work, and increases in the
proportion of people of working
age in the population, female
labour force participation
and educational attainment.9
Countries, including South Korea
and Thailand have capitalised on
this window of opportunity for
economic growth by investing
in the health, education and
welfare of their citizens. India
stands poised to benefit too
- by transforming the lives of
its people, optimising public
spending and bolstering the
global economy.
A matter of human rights
While it is important to
document the diverse social,
displaced women, sex-workers,
adolescents and young people,
religious and ethnic minorities
are all vulnerable groups whose
access to family planning is
limited. In an Indian context a
non-discriminatory approach
must also address young people.
Young people have age-specific
sexual and reproductive health
needs. Addressing their needs
will require trained family
planning counsellors, statutes
on privacy and confidentiality, an
emphasis on contraception and
disease prevention, approaches
reaching out to young
couples and comprehensive
sexuality education which
is grounded in human
rights and gender equality.
The right to the highest
attainable standard of health
|
|
3 Page 3 |
▲back to top |
Population Foundation of India
Policy Brief/2013
requires that everyone can
access health information and
services without restrictions.
However, in India the following
barriers obstruct women’s
access to family planning
services:
1. Lack of sufficient informa-
tion and counselling re-
strict women’s ability to
make free and informed
choices.
2. Lack of confidentiality
and privacy
3. Absence of adequate
choice and supply of a
wide range of contracep-
tive methods, particularly
spacing methods.
4. Insufficient
providers.
trained
5. Little emphasis on spacing
methods, leading women
to rely on permanent
methods.
6. Poor quality of care in
family planning services.
Putting in place policies and
practices to remove these
barriers will contribute greatly
to increasing access to family
planning in India.
Human rights standards require
that a wide range of safe and
effective contraceptive services
be continuously available.
India has not introduced a new
contraceptive method in the
public sector in over 40 years,
since IUCDs were included in
1965.12 A number of methods
are either unavailable in the
public sector basket of choices,
or lack trained personnel
who can counsel and deliver
these methods with adequate
standards of care. Moreover,
the restricted access to several
methods only in the private
sector, violates the human rights
principles of equitable access
to life saving technologies.
A pro-woman, human rights
approach to family planning
would ensure access to a larger
The UN recognizes that “for every US dollar spent
in family planning, between US$2 and US$6 can be
saved in interventions aimed at achieving other de-
velopment goals.”14
and more complete range of
contraceptives.
This could be achieved by
investing in client-centred
quality of care approaches. This
includes elements of choice
of contraceptive methods;
accurate information about
the effectiveness, risk and
benefits of different methods;
technical competence of
providers; provision of related
family planning services;
improved
provider-user
relationships based on respect
for informed choice; privacy
and confidentiality; and follow-
up.13 Studies have shown that
where clients feel that they are
receiving good care, rates of
contraceptive use are higher,
than in areas where women
are given lower quality of
healthcare.14
The International Conference
on Population and Development
(ICPD) Programme of Action
called for an approach that
is voluntary and adheres to
principles of human rights,
freedom from coercion and
individual decision-making.
Even though India is a signatory
of ICPD, and the National
Population Policy 2000 is
completely in tandem with
the ICPD approach, the driving
force behind many of the state
policies are still demographic
targets, population control
objectives and incentives and
disincentives.15 This approach
needs to be revised in line
with principles of social justice
and equity. The states need to
revise policies in line with ICPD
standards. One way to do this
is to discourage targets and
emphasise better choice and
information in contraceptive
options so that women are able
to exercise their freedom to
choose the method that best
suits their needs.
Reproductive choice is one of
the most fundamental human
rights and by freeing women
from an incessant cycle of
pregnancy, breastfeeding and
childcare, family planning
represents a giant step towards
gender equality .
|
|
4 Page 4 |
▲back to top |
Policy Brief/2013
Population Foundation of India
Reproductive choice is one of the most fundamental human rights and by free-
ing women from an incessant cycle of pregnancy, breastfeeding and childcare,
family planning represents a giant step towards gender equality.
Recommendations: Every Family a Planned Family
The way forward is to enable universal and voluntary family planning. Despite variations in
context and progress many of the broad factors are strikingly similar.
• Provide universal access to comprehensive family planning services to all women and men
(married, unmarried, adolescents, especially the poor and marginalised).
• Make available a wide choice of safe and effective modern contraceptives available at all
private and public health facilities.
• Strengthen the capacity of the health system to deliver a wide range of contraceptives
i. By providing quality training and capacity building of frontline healthcare providers,
ASHAs, ANMs, nurses, doctors, family planning counsellors. Healthcare workers must
be trained to exercise respect for the privacy and individual choices of their clients.
ii. Provide healthcare centres (PHCs, CHCs, District Hospitals etc) that are safe, clean and
easily accessible for ALL clients.
• Promote a community based approach to family planning. Directly involving communities
helps to prevent the stigmatisation of contraceptive use. Services must also ensure male
involvement and support for family planning decisions.
• Provide financial support in the form of state subsidies, national insurance schemes, gov-
ernment funding for family planning to ensure access for people who might otherwise
not be able to afford services. Increase donor and government funding to family planning
programs and encourage public/private partnerships to meet the enormous unmet need
in the country.
All of these factors would contribute to providing a comprehensive ‘package’ of sexual and re-
productive health services which place women and clients at the very centre.
Population Foundation of India
B-28 Qutab Institutional Area
New Delhi - 110 016
References
1 Census of India. 2011, Sample Registration System.
http://censusindia.gov.in/2011-Common/srs.html
2 Ministry of Health and Family Welfare, Government
of India, International Institute for Population Sciences
(IIPS) and Macro International. 2007. National Family
Health Survey (NFHS - 3), 2005-06: India: Volume I,
Mumbai: IIPS.
3 Singh S. et al. 2009. Barriers to Safe Motherhood in
India. New York: Guttmacher Institute.
4 UNDP. 2011 Millennium Development Goals: India
Country Report 2011. http://www.undp.org/content/
dam/undp/library/MDG/english/MDG%20Country%20
Reports/India/MDG_India_2011.pdf
5 Ibid.
6 Ministry of Health and Family Welfare, Government of
India & International Institute for Population Sciences
(IIPS). 2008. District Level Household and Facility Survey
2007-08. Mumbai: IIPS. In India this figure refers only
to currently married women who have indicated they
have an unmet need.
7 Cleland J. et al. 2012. Contraception and Health.
Lancet 2012. Published online July 10, http://dx.doi.
org/10.1016/S0140-6736(12)60609-6.
8 UN Population Division. 2009. What would it take
to accelerate fertility decline in the least developed
countries? Policy Brief, No. 2009/1
9 Canning D. & TP Schultz. 2012. The Economic
Consequences of Reproductive Health and Family
Planning. Lancet 2012. Published online July 10, http://
dx.doi.org/10.1016/S0140-6736(12)60827-7.
10 Cottingham J. et al. 2012. Use of Human Rights to
Meet the Unmet Need for Family Planning. Lancet 2012.
Published Online July 10, http://dx.doi.org/10.1016/
S0140-6736(12)60732-6.
11 Ibid.
12 The first IUCD to be introduced in the public sector
was Lippes Loop in 1965.
13 Cottingham et al. 2012 .
14 Koenig, MA. 2003. The Impact of Quality of care on
Contraceptive Use: Evidence From Longitudinal Data
from Rural Bangladesh. Baltimore: Johns Hopkins
University.
15 Sen, G. & A. Iyer. Incentives and Disincentives:
Necessary, effective, just? Seminar (web-edition). New
Delhi.