





 |
PIP Policy Brief_A Review of Planning_Budgeting_and Expenditure for Family Planning_under National Health Mission |
|
|
1 Page 1 |
▲back to top |
Policy Brief I December 2018
A Review of Planning, Budgeting
and Expenditure for Family Planning
under National Health Mission
Investments by the government in family planning are critical for population stabilization, thereby improving maternal
and child health, and fostering growth of the nation. A study commissioned by Population Foundation of India (PFI) -
“Planning, Budgeting and Expenditure for Family Planning under National Health Mission: A Review”
- analyses budget allocations for family planning activities under the National Health Mission in 18 High Focus States
(HFS)1, and its spending in Bihar and Uttar Pradesh. The study reveals that while allocations for family planning have
increased over time with variations between states, its utilisation tends to be much slower paced. It lays forth the
reasons behind inadequate allocations and expenditure, captures best practices, and suggests potential solutions in terms
of policy and programme actions to augment spending and more efficient utilisation of family planning resources.
Background
The Family Planning (FP) Programme in India rests on a rights-
based voluntary approach to meet the reproductive health needs
of its people. At the global level, India has pledged to provide
universal access to reproductive health services including FP
services by 2030 as a signatory of the Sustainable Development
Goals. It has also committed to investing $3 billion by 20202 at
the FP2020 Summit. In 2016, the Government of India expanded
the basket of choice for contraceptives in the public health
system from five to eight, with the addition of Centchroman,
Progestin Only Pills (POPs) and the injectable contraceptive Depot
Medroxyprogesterone Acetate (DMPA).
47.8%
Modern
contraceptive use
75.3%
Female sterilisation,
of all modern
contraceptive methods
13%
Unmet need for
contraception
(NFHS-4)
This translates to
30 million women
who wish to delay or avoid
pregnancy but do not have
access to contraceptives
(calculated from Census 2011 data)
The study
The study “Planning, Budgeting and Expenditure for Family
Planning under National Health Mission: A Review” examines
trends in the proposed and approved budgets for FP activities. It
covered three Financial Years – 2014-15, 2015-16 and 2016-17
and spanned 18 High Focus Large States, including the North
Eastern states, together accounting for almost 60% of the total
National Health Mission (NHM) allocations. The study reviewed
the current allocation and spending for FP and analysed shortfalls
in implementation. The districts of Gaya and Araria in Bihar
and Faizabad and Barabanki in Uttar Pradesh were chosen for
a deeper analysis to understand the reasons for low allocations
and expenditure.
Findings
Trends in budget allocations for family planning –
an analysis of 18 High Focus States
The trends in budget allocation for family planning reveal that on
an average, the High Focus Large States (HFLS) allocate 4 % of
their NHM budgets for family planning while the North Eastern
states allocate 2%. The budgets for FP in the HFLS increased by
46% (Rs. 515 crores to Rs. 752 crores) between 2014-15 and
2016-17 in comparison to the High Focus North East (HFNE)
states, where the increase has been marginal.
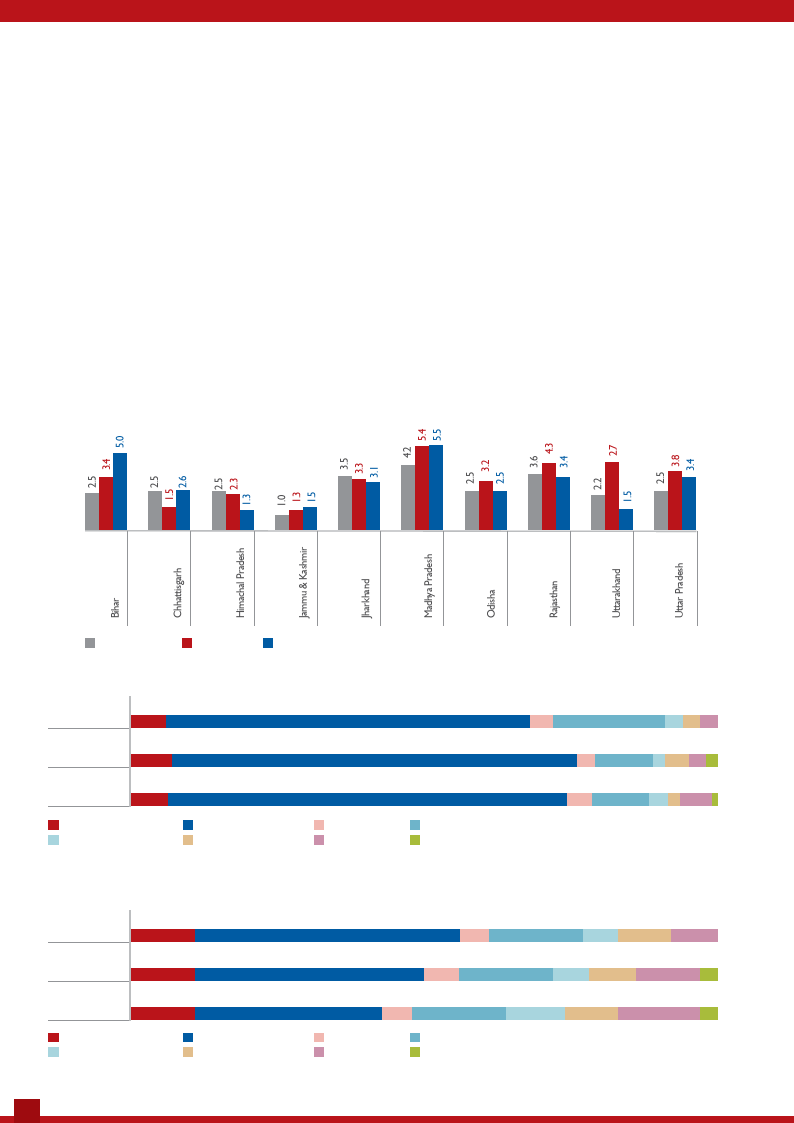
An inter-state analysis of trends in the share of proposed NHM
budgets for family planning in the HFLS for the three Financial
Years shows a wide variation that ranges between 1.0% and 5.5%
(Fig.1). While there is an increase in most (seven out of ten) of
the HFLS in 2015-16, these are inconsistent, except in Bihar and
Madhya Pradesh, where the proposed FP budgets have increased
steadily over the years. In Jharkhand and Himachal Pradesh,
the budget proposals for FP declined. Lower budget proposals
are also evident in Uttar Pradesh (3.4%), Odisha (2.5%) and
Rajasthan (3.4%) in 2016-17.
Among the High Focus North East states (HFNE), Assam is the
only one that has consistently proposed higher budgets for family
planning since 2014-15. Declining trends for FP in budget proposals
were observed in at least 50% of the HFNE states in 2016-17.
1 Arunachal Pradesh, Assam, Bihar, Chhattisgarh, Himachal Pradesh, Jammu & Kashmir, Jharkhand, Madhya Pradesh, Manipur, Meghalaya, Mizoram, Nagaland, Odisha, Rajasthan, Sikkim, Tripura,
Uttarakhand, Uttar Pradesh
2 FP2020 London Summit, India Country Report, July 2017
1
|
|
2 Page 2 |
▲back to top |
Trends in approval of family planning budgets
The Centre’s priority to family planning activities is reflected in the
approval rates of the budgets proposed by the states. In 2016-17,
more than 90% of the FP budgets proposed were approved by the
Centre in 11 of the 18 High Focus States. Uttar Pradesh is the only
HFLS that received a lower approval (76%). However, the North
Eastern states, with the exception of Sikkim and Mizoram, have
lower approvals.
Trends in composition of family planning budget
The HFLS allocated close to 70% of their family planning budgets
for limiting methods of contraception, including female sterilisation
and Non-Scalpel Vasectomy, compensation for female and male
sterilisation and accreditation of private providers for sterilisation
services (Fig. 2). 10% of the budget in these states is allocated for
incentives to ASHAs and FP counsellors. Spacing methods received
a low allocation of 3-4% of the total FP budget in the HFLS states,
while in the HFNE states, the allocation for spacing ranges between
5-6% (Fig. 3). HFNE states prioritise provider incentives (16%), drugs
and supplies (14%), training (9%) and IEC/BCC activities (10%).
Allocation of family planning budgets
An analysis of the FP budgets reveal the skew towards limiting
methods i.e. female sterilisation. Budget allocations in the HFLS for
spacing have fluctuated between 3% and 4% between 2014-15 and
2016 -17, and for limiting methods has increased from 62% to 68%
between 2014 -15 and 2016 -17. Being a young country with 27.5%
of its population in the 15-29 age group (Census 2011), India needs
to focus on methods for delaying or spacing births, rather than
permanent methods. The current funding of family planning
activities may not fulfil the needs of over half our population in the
reproductive age.
In addition, budget allocations towards training of health personnel
and promoting social and individual behaviour change through
communication in the HFLS have remained constant at 3%
during the years under review. In fact, allocations for training
have declined further in recent budgets, even though there is an
evident need for capacity building of health workers on the new
contraceptive methods.
Figure 1: FP Proposed Budget as a percent of Total NHM Proposed: High Focus Large States
FY 2014-15
FY 2015-16
FY 2016-17
Source: RoPs with supplementaries, NHM, GoI.
2014 - 15
6
Figure 2: Composition of FP budget (in percent) - HFLS
62
4
19
333
7
2015 - 16
71
3
10
2 3 32
6
68
2016 - 17
4
9
32 5 1
Miscellaneous
BCC/IEC Activities (FP++)
Terminal/Limiting Methods
Training
Source: RoPs with supplementaries, NHM, GoI.
Spacing Methods
Drugs & Supplies
Incentives (Performance Incentives for RMNCH/FP Counsellors and ASHAs
Salaries(IEC Coordinator,RMNCH/FP Counsellors
2014 - 15
11
Figure 3: Composition of FP budget (in percent) - HFNE
45
5
16
6
9
8
11
2015 - 16
39
6
16
6
8
11
3
11
2016 - 17
32
5
16
10
9
14
3
Miscellaneous
Terminal/Limiting Methods
BCC/IEC Activities (FP++)
Training
Source: RoPs with supplementaries, NHM, GoI.
Spacing Methods
Drugs & Supplies
Incentives (Performance Incentives for RMNCH/FP Counsellors and ASHAs
Salaries(IEC Coordinator,RMNCH/FP Counsellors
2
|
|
3 Page 3 |
▲back to top |
In comparison, the HFNE states seem to have shifted priorities
in family planning resource allocation, with budgets for limiting
methods declining from 45% in 2014-15 to 32% in 2016-17.
Higher allocations are made for spacing methods, IEC/BCC
activities, FP training and provision of drugs and supplies in HFNE
states.
Spending of family planning budgets in Uttar
Pradesh and Bihar
The spending of family planning budgets is sub-optimal in both
Bihar and UP, which utilised 55% and 34% respectively of the
allocated budgets in 2016-17.
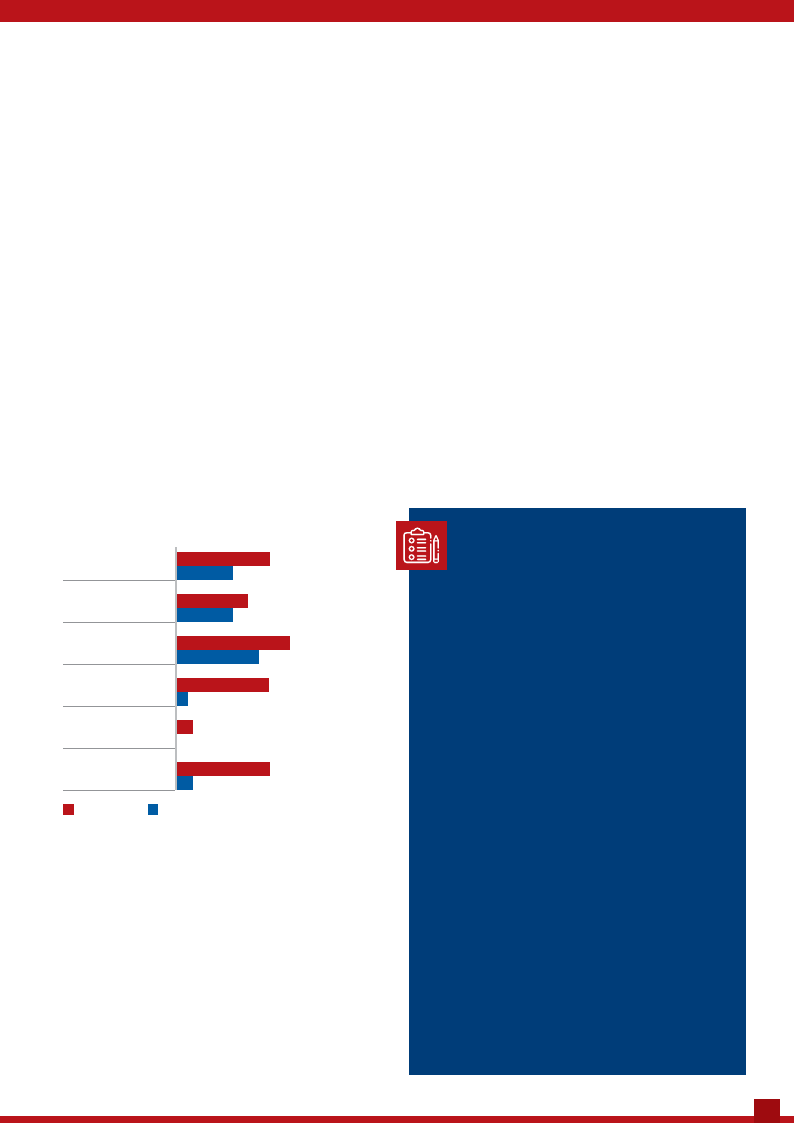
Similar to allocations, the spending for family planning activities
is also skewed towards limiting methods and incentives to
frontline health workers. In Bihar, while 82% of the budgets are
assigned to limiting methods, just 58% is utilised; in UP, of the
60% budget allocated for limiting methods (Fig. 4), only 35%
is used. About 50-70% of the money available for incentives
gets utilised. However, spending on spacing methods is very
low. Just 35 to 44% of the allocated budgets are utilised in UP
and Bihar respectively. Similarly, only 10% of allocations for
IEC/BCC activities was spent in Bihar; in UP the funds for this
activity remained unutilised in 2016-17. Utilisation of budgets for
training also remains low, especially in UP where only 7% of the
allocated budget was spent. These figures indicate a dissonance
with current requirements based on India’s demographic profile,
and are likely to have an impact on the uptake of the new
contraceptives introduced in public health facilities.
increase over the previous year’s budget. Therefore, districts
remain unaware of the money they are likely to receive and
fail to strategise their spending.
ÆÆ Delays in PIP approvals and release of funds: Although
the preparation of PIPs for the next Financial Year are
initiated in the third quarter of the current year, they get
approved during the second quarter of the next financial
year, with a gap of six to nine months. About 53% of
approved funds are released more than a year after the
planning has taken place, leaving hardly any time for the
districts to spend the money as per their needs.
ÆÆ Inadequate data management systems: Systematic
processes to monitor and track progress in fund utilisation
are not available at the state and district levels.
ÆÆ Lack of integration in accounting systems: Different
accounting standards between the treasury and the Public
Financial Management System result in transparency and
accountability issues, thereby making it difficult to track
disbursements and the use of funds.
ÆÆ Low priority for family planning: Districts are directed
to concentrate spending on priority programmes such as
the Janani Suraksha Yojana within the NHM, which does
not have a ceiling on spending. As a result, family planning
activities are often set aside and there is no clear strategy
for focused spending of family planning budgets.
Figure 4: Utilisation of budgets for family planning
activities in 2016-17 (in percent)
Limiting Methods
58
35
Spacing Methods
Asha Incentives
44
35
70
51
FP Training
57
7
BCC/IEC Activities
10
0
Procurement of FP
58
Equipment
10
Bihar
Uttar Pradesh
Common challenges in planning, allocation and
spending family planning budgets
The study noted several constraints that hinder family planning
budget allocations, resource availability and spending in Bihar and
Uttar Pradesh:
ÆÆ Limited decentralised planning: The district level
planning process which requires the consolidation of
resource requirements at the village, block and district
levels appears to be weak in these states. As a result, there
is no analysis of expenditure on family planning activities.
PIP budget proposals continue to be prepared at the state
level using an incremental budgeting approach, with a 10%
Recommended actions
Specific action points to strengthen activities related to the
planning, allocation and utilisation of family planning budgets
include:
1. Need-based budgets aligned with per capita
eligible population: The current budgetary allocations
for family planning need to be revisited and planned
in accordance with the reproductive health and
family planning needs of the districts’ eligible couple
population. Most importantly, states need to prioritise
and devise mechanisms to plan and budget for unmet
need for family planning.
2. Increase resource envelope for spacing methods:
As against the current allocation trends, it is necessary
to increase allocations for spacing methods and
components such as IEC/BCC and training. These are
critical to expanding the availability of the three new
spacing methods introduced into the public health
system in addition to those that already exist.
3. Separate training on PIP planning and budgeting
at the decentralised level: State PIPs need to
appropriately reflect the priorities and financial needs
of family planning at the block and district levels. It is
imperative to build the capacities of concerned officials
at these levels in developing plans and preparing budgets
for family planning activities that will eventually be
reflected in the budget proposals of the state.
3
|
|
4 Page 4 |
▲back to top |
4. Strengthen capacity of districts to plan and
operationalise family planning budgets: There is a time
lag between the approval of budgets and their arrival at the
districts. Hence, there is a window of at least three to four
months with the district and this time should be used to
prioritise and plan for family planning activities proposed
in the PIP. This will ensure that the district is prepared
to operationalise the planned activities immediately on
receipt of funds from the State Health Society.
5. Integrate financial management systems into a single
platform: Different financial management standards
between the treasury and the PFMS result in poor
transparency and accountability, thereby making it difficult
to track disbursements and the use of funds. There is
therefore a need to streamline the financial systems and
integrate them with the PFMS at the district level, so that
funds for family planning can be tracked right from the
stage of disbursement to their last point of use.
6. Regular tracking of fund availability to facilitate
optimal use: Poor quality of data and gaps in them
results in lack of evidence for planning and monitoring.
Differences in formats and repeated adjustments through
the year make it difficult to track fund flows and ensure
accountability. Institutionalising better data management
systems and strengthening the existing ones will enable
better decision-making and the optimal utilisation of
available budgets.
Changes in spending family planning
budgets after the study period
After the launch of Mission Parivar Vikas, that aims to
increase access to contraceptive and family planning services
in 146 High Focus Districts, there has been a change in
spending patterns. The utilisation of family planning budgets
in Uttar Pradesh have increased from 39% in 2016 -17 to
66% in 2017-18, and in Bihar from 57% to 62% during this
period. Discussions with the Chief Medical Officers (CMOs)
and District Programme Managers in Uttar Pradesh revealed
a few positive steps taken to expedite utilisation of FP
budgets in 2017-18.
The positive steps that have helped in improved utilisation
in Uttar Pradesh are:
ÆÆ Acceleration of PIP approval processes from the
Centre, making funds for family planning available in
the first quarter
ÆÆ Clear communication from the state Mission Director,
NHM to the CMOs of all districts directing them to
ensure 100% utilisation of the approved family planning
budgets
ÆÆ Providing funds on a quarterly basis to the districts so
that regular activities can continue
ÆÆ Sustained monitoring leading to increased spending on
several family planning activities
ÆÆ Enhanced autonomy and flexibility in making approvals
at the district level by CMOs
Best practices in planning, allocation and spending family planning budgets
It was observed that Tamil Nadu, Uttarakhand and Madhya Pradesh had better spending rates in the period from 2014-15 to 2017-18
as compared to Bihar and Uttar Pradesh. Some of the promising practices that emerged through discussions with state NHM officials
in charge of family planning in these three states are detailed below:
Planning and budgeting process
ÆÆ Family planning budgets
are prepared realistically in
line with the eligible couple
population distribution;
budgets in the PIP are
proposed on the basis of
their spending capacities.
ÆÆ Focused training on
planning and budgeting
activities in the PIP,
including budgeting for
family planning activities,
has been provided to block
and district level officials.
As the demand for family
planning services increased,
the states proposed higher
amounts in their PIPs and
got them approved from
the Centre.
Spending mechanisms
ÆÆ At the start of the Financial Year, letters and
guidelines are issued from the State Health Society to
the District Health Societies with intimation of funds
approved to ensure seamless utilisation.
ÆÆ Direct financial powers with implementing units
(Primary Health Centres, Community Health Centres,
Sub-district hospital, District Hospital) through
the District Health Society and Patient Welfare
Societies have delinked the approval process from
district authorities and enabled increased spending in
accordance with local needs.
ÆÆ Decentralised delegation of financial powers has
helped expedite spending and make timely payments.
Direct Benefit Transfers through the PFMS at the
block level have ensured that incentives reach
beneficiaries and frontline health workers on time.
ÆÆ CMOs approve regular activities in concurrence with
the District Health Society. This enables the districts
to carry out the activities and book the expenditures
simultaneously, thereby ensuring a balance between
physical and financial outputs.
Review mechanism
ÆÆ Periodic financial and physical
review meetings at the district
and state levels are conducted to
simultaneously track the activities
undertaken and their related
expenditures. This includes
comprehensive financial reviews
of disbursements through the
PFMS and FMRs on a monthly
basis. The review process has
enabled the states to spot gaps
and address them in a time bound
manner.
ÆÆ Block-wise reviews helped to
identify the blocks that performed
well and those that did not. The
better performing blocks are
incentivised through additional
funds, while the least performing
ones are penalised for under-
spending by reducing their
disbursements.
Population Foundation of India: B-28, Qutab Institutional Area, New Delhi - 110016 I T: +91 11 43894 100 I F: +91 11 43894 199
4