





 |
CAH Briefer 1 Health and Wellness Centres in Assam_English |
|
|
1 Page 1 |
▲back to top |
COMMUNITY ACTION
FOR HEALTH
Bringing public into public health
Empowering the community to actively
engage and monitor services at Health
and Wellness Centres in Assam
Secretariat
Advisory Group on Community Action
#1
ASSAM
An intervention to bolster
community mobilisation
and monitoring of HWCs
7 aspirational districts,
222 HWCs
India’s commitment to quality, accessible care has received a further boost with the
ambitious Ayushman Bharat scheme to provide comprehensive primary health care
through Health and Wellness Centres (HWCs) across the country. As India strides
towards its year 2022 goal of upgrading 1,50,000 existing Sub Health Centres (SHCs),
Primary Health Centres (PHCs) and Urban Primary Health Centres (UPHCs) into
HWCs, it is crucial that people be at the centre of this change. Local communities
must be involved to ensure that the public health system makes quality care available
and accessible to fulfil people’s health needs.
Community Action for Health (CAH), a key strategy under the National Health
Mission (NHM), Government of India, has demonstrated an innovative approach in
Assam to promote community mobilisation and monitoring of HWCs. Its pilot has
showcased a simple but effective strategy to secure the community’s participation
in accessing and demanding services, monitoring the availability to services and
providing feedback, thereby facilitating improvements in the quality of health care.
This brief summarizes the processes adopted to strengthen community mobilization
and monitoring of HWCs and how the community’s feedback led to corrective actions
on the ground.
|
|
2 Page 2 |
▲back to top |

THE ASSAM PILOT
An intervention for community mobilisation and
monitoring of Health and Wellness Centres
CONTEXT
Assam initiated community-based monitoring in 2007.
Currently, CAH implementation in the state focuses on
seven aspirational districts: Baska, Barpeta, Darrang,
Dhubri, Goalpara, Hailakandi and Udalguri, covering a
total of 55 blocks with 1,110 Village Health, Sanitation
and Nutrition Committees (VHSNCs).
Assam is establishing 1,720 HWCs at the Sub Health
Centre level. During the pilot’s implementation (2018–
19), 222 of these HWCs were set up in the seven
aspirational districts. The state NHM designed and
piloted a community-side intervention under CAH to
mobilise the community and promote their active
involvement in the formative stages of HWCs. The pilot
was implemented by the State Community Processes
Unit (SCPU) in December 2018. The Advisory Group on
Community Action (AGCA) gave support to the pilot by
guiding the implementation processes, designing tools
and co-facilitating training of trainers with NHM.
INTERVENTION
The pilot intervention focused on building the
community’s capacity to monitor how well the HWCs
are functioning and what gaps and issues need to be
addressed to ensure people receive the intended quality
of comprehensive primary health care at HWCs. The key
steps of the intervention are listed below:
A. Preparatory and facilitative processes
1. Development of a tool kit: A tool kit was developed
to build VHSNC members’ awareness about what
services are available at HWCs and how feedback
can be collected on the functioning of HWCs and the
issues being faced by patients. The tool kit was
made available in English and two local languages
(Assamese and Bengali).
2. Creation of a pool of master trainers at the district
level: Thirty-four personnel, including Block
Community Mobilisers, ASHA Supervisors and
Assistant Block Programme Managers, were trained
as master trainers. The training was facilitated by
SCPU and AGCA.
Health and Wellness Centres represent India’s bold commitment to secure comprehensive,
quality health care at the primary level. Active engagement of communities will be crucial to
achieve the goal of improving the availability of and access to quality health care by people.
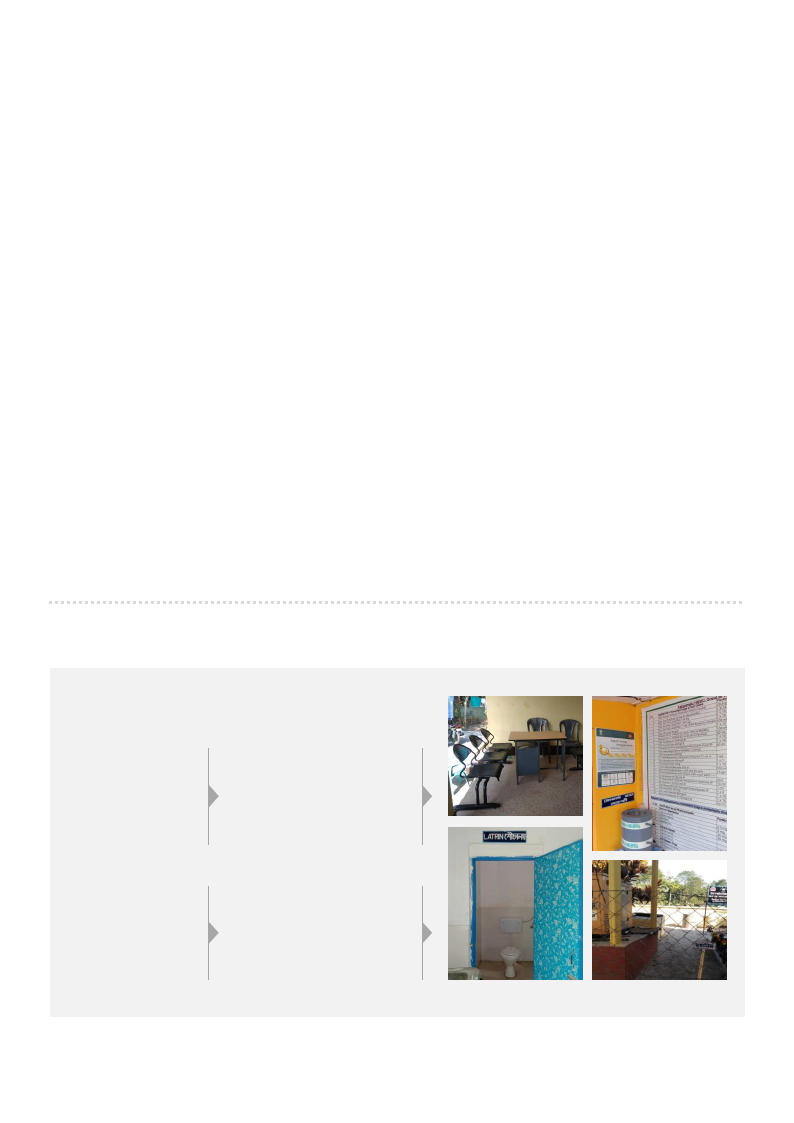
ENGAGING COMMUNITIES TO DEVELOP LOCALLY RESPONSIVE HEALTH CARE: A SNAPSHOT
Orientation of district
master trainers
Orientation of
VHSNC members
Patient feedback
is collected
VHSNC members hold
a dialogue with the
HWC’s Community
Health Officer and
ASHA Supervisor
VHSNC members monitor
services at an HWC
|
|
3 Page 3 |
▲back to top |
3. Creation and training of village-level feedback
teams: Local feedback teams at the village level
were developed to create awareness and seek
independent feedback about the functioning of
HWCs and the issues patients were facing. The
feedback team for an HWC comprised three active
members from each VHSNC falling in the catchment
area of the HWC. ANMs and ASHAs selected
feedback team members from among the
community representatives that were part of
VHSNCs, including panchayat members, young
mother’s groups, farmer’s groups, etc. A total of
3,200 VHSNC members were selected and trained to
collect feedback about HWCs’ functioning, the costs
being incurred by patients to get treatment, identify
gaps and conduct discussions with HWC staff to
find solutions.
B. Field implementation
4. Monitoring of HWCs and collection of feedback: The
feedback teams, comprising trained VHSNC members,
went to HWCs on a bi-monthly basis to identify gaps
and get patient feedback. Information was collected
and recorded on feedback forms about whether staff
such as Community Health Officer (CHO) and
Multipurpose Health Worker (MPW, male and female)
were available; whether the intended health services,
diagnostic tests, drugs and other commodities were
being provided to people; and whether facilities such
as a clean waiting area, a usable toilet and drinking
water were available. Feedback was collected from
patients about the behaviour of health staff and the
out-of-pocket expenses being incurred. The feedback
teams also held preliminary informal discussions with
the CHO, ANMs and MPW on the identified gaps and
sought ways to plug these gaps.
5. Analysis of feedback and action plan to fill the gaps:
The feedback teams held a focus group discussion
with the CHO and the HWC staff to discuss the
findings. An action plan was put in place, including the
corrective action(s) required to fill the gap(s), the
person/body responsible for the action and the
timeline for action. Data from different feedback forms
was fed into Google forms for compilation and
analysis at the state level to identify and analyse
critical issues.
IMPACT
Based on feedback from the community, the state NHM
Mission Director issued instructions to Joint Directors
at the district level to act on the gaps the community
had identified. Among the gaps highlighted by the
community at several HWCs were: infrastructural
issues like lack of power back-up, seating
arrangements and drinking water facility; irregular
supply of medicines; vacant positions of health staff
and need for labour room equipment. Informed by such
feedback from the ground, the concerned district
authorities are taking actions to resolve issues and
improve the quality of health care at HWCs. The
illustration below shows two examples of how
feedback from the ground has led to corrective actions.
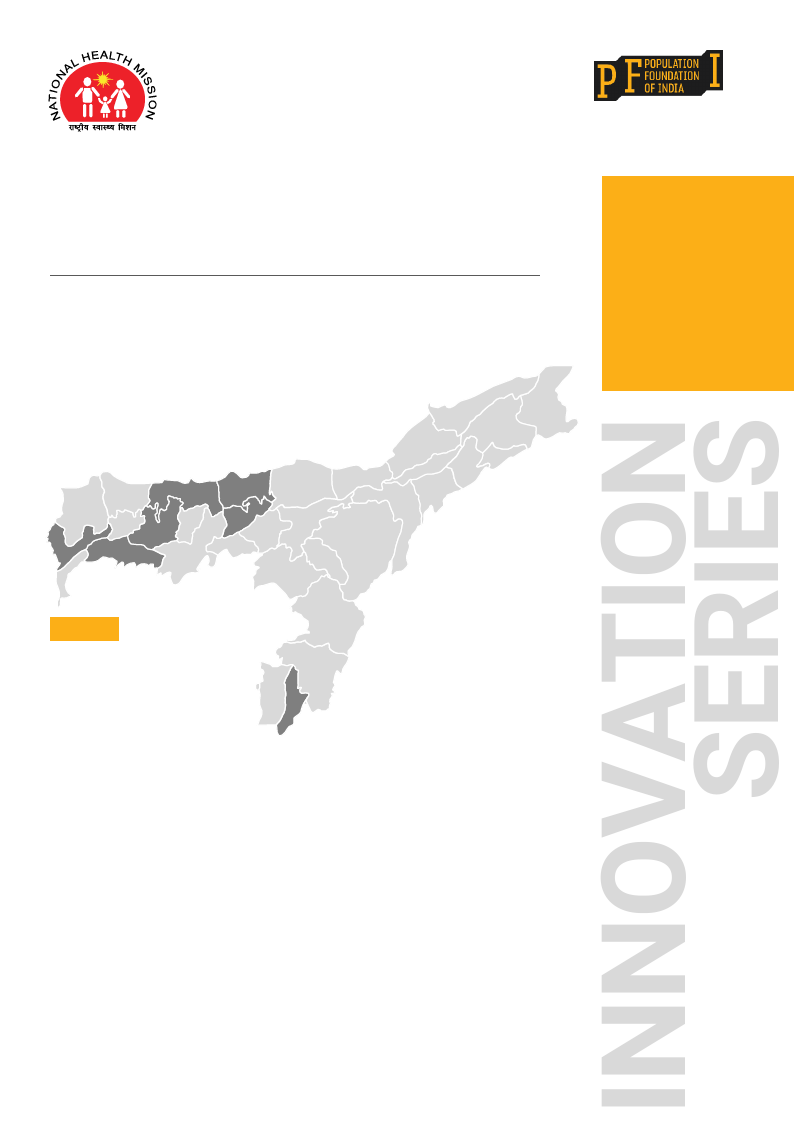
COMMUNITY FEEDBACK PROMPTS CORRECTIVE ACTIONS: A FEW EXAMPLES
ISSUES
HIGHLIGHTED BY
THE COMMUNITY
Irregular supply of
essential drugs
CORRECTIVE ACTIONS
Letter issued by the Office of
the Joint Director of Health
Services, NHM, Goalpara
district, to drug management
personnel to ensure proper
flow of essential drugs to HWCs
Lack of power
back-up facility,
inadequate provisions
for waiting area and
drinking water supply
Office of the Joint Director
of Health Services, NHM,
Udalguri district, ensured
repair of the generator and
setting up of waiting area
and drinking water facilities
|
|
4 Page 4 |
▲back to top |
BRINGING COMMUNITY VOICE INTO HEALTH SERVICE DELIVERY
COMMUNITY MEMBERS SHARE THEIR FEEDBACK ON
AN HWC IN ORANG BLOCK, UDALGURI DISTRICT, ASSAM
“ The community of this village and the hospital staff are
committed and working together to improve this Health and
Wellness Centre. Things have really changed at this HWC, and
we are happy with the services provided.”
“ The doctor is available 24-hours and we get consultations,
medicines and tests. If the ultrasound and X-ray facility could
also be made available here and also some small things, like a
few more chairs and racks to keep medicines, this HWC will
become even better.”
“ Although this HWC is for four villages, people from at least six to
seven adjoining villages, and even far off villages, come here for
delivery. It is because the doctor here is always present and the
staff is very dedicated.”
“ The onset of summer brings several ailments. The doctor here
gives good attention to everyone, but his workload is too much…
About 25–30 deliveries are conducted at this HWC every month!
An additional doctor is needed here to share this workload.”
LESSONS LEARNED
• Identification of real issues on the ground requires
independent feedback from the community. Creation of
a village cadre — feedback team — that was devoid of
frontline health workers and HWC staff allowed real,
unbiased information about gaps and issues to emerge.
• Empowering and training community members to take
up the responsibility of monitoring health services gave
them a sense of ownership, pride and confidence, which
are critical to foster active community engagement.
• Mentoringand continuous engagement can help lay the
foundation for mutual trust between health functionaries
and the community. The state, district and block NHM
teams owned the processes and supported the initiative
to promote community participation.
• Providing the community members with an easy-to-
use tool kit, as provided by the pilot, can motivate and
enable them to contribute effectively. The illustrated
tool kit was easy to understand and use and served as
a composite resource that built the community’s
awareness and enabled assessment of HWC services,
collection of patient feedback, and discussion with
HWC staff to plug the identified gaps. It, thus, proved to
be a useful mechanism to bring in the various steps of
monitoring, which reduced delays in initiating
corrective actions.
• Prompt redressal of the issues raised is necessary to
keep up the motivation and interest of the community.
THE WAY FORWARD
The intervention has demonstrated its effectiveness in
securing community participation to improve the quality
of local health service delivery. In FY2020–21, Assam will
scale up the intervention to 58 more HWCs in the seven
aspirational districts. Some key aspects of the intervention,
such as an in-house pool of master trainers and a tested
tool kit, augur well for scaling up this initiative in other
states as well. All the states already have ASHA and
VHSNC trainers at the district and block levels, and this
resource could be leveraged to roll out the intervention
swiftly and efficiently.
Secretariat
Advisory Group on Community Action
B-28, Qutab Institutional Area, New Delhi – 110016
T: +91 11 43894 100; +91 11 43894 199
www.nrhmcommunityaction.org | www.populationfoundation.in