





 |
Focus 1988 October - December |
|
|
1 Page 1 |
▲back to top |
Bulletin of Family Planning Foundation, Volume II, No.4 October-December , 1988
to National Seminar Qn Infant Mortality in R~lation Fertility
Agenda for Action on the Anvil
The Family Planning Foundation organised on July 1 and 2, 1988,
a Nationa I Seminar on Infant Mortality in Relation to Fertility to focus
attention on how high infant mortality and fertility are inter-related and
causative of each other. The seminar threw up a number of sugges-
<'<.> tions and recommendations which are now being discussed with the
experts to prepare praCilciiraciion pial1s for [implementation in the field.
The deliberations of the Seminar which was inaugurated by Mr. J. R. D.
Tata, Chairman of the Foundation on July 1, and chaired by Dr. Harcharan
Singh, Adviser, Planning Commission, on July 2, will also be of help
in the formulation of the Health and Family Welfare segment of the Eighth
Five-Year Plan.
We present here a very brief summary of the proceedings of the seminar
which discussed threadbare the findings of the Project on Infant
Mortality in Relation to Fertility conducted in five States of India as
a collaborative venture between International Development Research
Centre (IDRC), Canada and Family Planning Foundation (FPF), New
Delhi (Details of the Project were reported in our last issue).
from 103 to 41 and the fertility
rate from 6.3 to 3. NeaJer home,
Kerala which had the lowest IMR
of 27 among Indian States, also
had the lowest birth rate.
Tragic Situation
Drawing attention to the serious-
ness of infant mortality problem in
India, Mr. Tata said that out of 26
million children born every year,
2.5 million or 95 out of every
Welcoming the participants,
Mr. Harish Khanna, Executive
Director, Family Planning Founda-
tion, introduced the theme and
outlined the programme of the
national seminar. He said that the
purpose of the seminar was not
only to share the findings of the
FPF-IDRC project on Infant Morta-
lity in Relation to Fertility but also
to provide useful inputs into the
Eighth Plan and demonstrate
through experimentation on a pilot
basis the efficacy and effective-
ness of appropriate interventions
aimed at reducing infant mortality
and ultimately fertility at the re-
quired speed so as to achieve the
national goal Le., 1MR of 60 and
NRR-1 by 2000 A.D. He ex-
pressed the hope that the presence
of many eminent national and
international experts would help
evolve the basic design of a new
strategy which could cope with
the problem in the next decade
or so.
In his inaugural address,
Mr. J. R. D. Tata said that the
importance of infant mortality as a
deterrent to the wider adoption
of family planning measures had
not been adequately understood
or appreciated so far. There was
a symbiotic relationship between
infant mortality rate and birth rate;
higher infant mortality invariably
meant higher birth rate and vice
versa.
Mr. Tata said that in many Third
World countries, reduction of child
mortality rates had contributed to
reduced population growth. In this
context, he cited the example of
Thailand where, between 1960 and
1986, infant mortality rate dropped
The serious dimensions of our
population problem need our
undivided and urgent attention.
Sustained governmental efforts
have to be backed up by people's
participation to make a success
of programmes in this area.
- From Prime Minister Rajiv
Gandhi's letter of 14th June,
1988 to Mr. J. R. D. Tata.
|
|
2 Page 2 |
▲back to top |
Mr. J.R.o. Tata
delivering the
inaugural
address.
Dr. (Mrs.) Nina Ranjan, Director
of National Institute of Public Co-
operation and Child Development,
observed that in view of the magni-
tude of the problem, it was diffi-
cult to make much headway unless
local community participation, peo-
ple's cooperation and involvement
of voluntary organisations were
ensured.
Redefine the Targets
thousand, died before completing Root Causes
their first year and nearly 8 million
Mrs. Avabai B. Wadia, President,
died before reaching the age of 5, Family Planning Association of
as against only 5 per cent in India, observed that the root causes
developed countries. This indeed of high infant mortality and ferti-
was a tragic situation which was lity, particularly in Northern States
made all the more tragic by the and the vulnerable sections of
fact that many of these infant society, were ignorance about
deaths occurred amongst poorer health and safe and convenient
families due to diseases for which family planning interventions,
prevention or cure have long been which were available, as also un-
available.
willingness to use and profit from
What was needed today in this counsel, and inability to pay for
regard was a more vigorous pur- the services. She pleaded that
suit of the objectives of the child reduction in maternal and infant
survival movement. Experience in mortality and adoption of smaII
the 1980s had shown that through family norm must be the main
the Child Survival and Develop- thrust of the health sector in the
ment Revolution, India was cap- Eighth Plan.
able of dramatic improvements
with in a short period of five to ten
years as a result of the synergy of
Dr. Shanti Ghosh, Paediatrician,
said that if they did not attack
root causes of maternal and child
low cost-high impact medical mortality and give enough im-
technologies, capable of prevent-
ing a majority of premature deaths,
he concluded.
portance to promotive and pre-
ventive aspects of maternal and
child health, including family plann-
Mr. S. S. Dhanoa, the then ing, neither the infant mortality
Health Secretary, Ministry of Health nor fertility rate would fall. She
and Family Welfare shared his . pointed out the need for going
concern with others for distress- beyond the present child survival
ingly high infant mortality and strategy and for looking at maternal
fertility rates. He said that in spite
of statewise variations most of the
and child health as a single com-
posite unit so as to work out a
infant deaths were due to circum- package of services and inputs
stances leading to birth and death required for it.
that followed immediately. These
must be prevented. In this con-
Dr. (Mrs.) Sudha Tewari, Manag-
text, he emphasised the impor- ing Director, Parivar Seva Sanstha,
tance of education of mothers, underlined that reports had brought
training of Dais, dissemination of out rather consistently the risk to
simple health messages through child's life due to too early, too
person-to-person communication close, too many and too late
in the overall child survival revo- deliveries which must be prevent-
lution.
ed through family welfare services.
Prof. Ashish Bose, Director, Insti-
tute of Economic Growth, observed
that no civilized society could
afford to have an IMR above 100
and that there was nothing sacred
aboutthe IMR of GOto be achieved
by 200 A.D. In fact, 60 was not
enough; it should be 30, and it
was possible to achieve it with
known and already available inter-
fi vention~. What was needed was ..~. :l
to redefIne the targets and achieve
them with full determination and
commitment.
Dr. M. E. Khan from Operation
~esearch Group, Ahmedabad said
that behind most of the direct and
proximate causes of infant d,eaths,
the~ lay poverty, malnutrition,
ignorance, low status and high
work load of women and that
these root causes must be tackled
along with health and family wel-
fare problems.
Dr. Pravin Visaria, Director, The
Gujarat Institute of Area Planning,
Ahmedabad, emphasized the need
to work out priority areas of inter-
ventions rather carefully because
there were so many factors which
directly and indirectly affected in-
fant mort;! Iity.
Dr. K. Srinivasan, Director,
International Institute of Popula-
tion Sciences, pleaded for a judi-
cious combination of both econo-
mic and social interventions to
accelerate the required rate of re-
duction in infant mortality and
fertility.
Dr. V. K. Paul, from All India
Institute of Medical Sciences, asked
for restructuring of the entire pri-
mary health care system and adop-
(Contd. on Page 8)
|
|
3 Page 3 |
▲back to top |
A Comparative study of KeraJa and West Bengal
Factors Contributing to low Mortality in Kerala
!n States or regions with large
proportions of economically and
socially deprived people, interven-
tions aimed at. reducing mortality
should give higher priority to social
equity, Le., in the fields of educa-
tion, health, transport and so on,
than to economic equity. A decline
in the mortality rate can be ex-
pected to contribute towards
equity in economic development.
This view-point is presented by
Dr. Moni Nag, Senior Associate
with the Centre for Policy Studies,
The Population Council, New York,
in an article published in World
Health Forum (Vol. 9, No, 2,
1988).
* Greater Accessibility to Health
Facilities;
* More Equitable Distribution of
Educational Services;
* Higher Degree of Political
Awareness.
Equity in health care and educa-
of the situaticn in Kerala and
West Bengal.
The Infant Mortality Rate in 1982
was 32 in rural Kerala, 93 in rural
West Bengal, and J 14 in rural India
as a whole. The figures were
lower in urban areas: 24 for
Kerala, 52 for West Bengal and 65
for the entire country. The cYude
death rate in 1982 was 7 in 1'ural
Kerala, 12 in rural West Bengal and
13 in rural India.
Economic Factors
However, per capita income has
always been lower in Kerala than
West Bengal. The assumption that
the State's healthy demographic
trends were influenced by the com-
paratively more equitable distribu-
tion of income and assets, is not
borne by empirical studies, at least
until the end of the 1970s. On
the other hand, surveys conducted
by the Reserve Bank of India in
1961 and 1971 showed that the
distribution of land and total assets
Kerala might have made food con-
sumption more equitable there than
in other States, is also not supported
by the available data.
Health Services and
Their Utilization
As regards the number of beds
per 1,00,000 population in hos-
pitals and dispensaries, there has
-been no significant difference bet-
ween West Bengal and Kerala.
West Bengal has always had the
higher doctor/population ratio,
whereas Kerala has always had
the high nurse/population ratio.
Kerala and West Bengal differ little
in per capita government expendi-
ture on health, bul"more equitable
distribution of health services in
Kerala is reflected in its propor-
tionally higher spending on pri-
mary health centres and sub-
centres.
In both Kerala and West Bengal,
local medical facilities are popular,
particularly ••in rural areas. They
tion are undoubtedly important, but
underlying factors also have to be
taken into account, notably the
development of political awareness
in rural households was less equit-
able in KeraJa.thanmwest&ngal.
Finding no explanation for lower
mortality in rural Kerala in economic
are aided to some extent by the
State Governmepts but depend
mainly on the support of the
general public. However, there is
and the action among the masses,
according to Dr. Nag, who has
come to these conclusions after
examining the areas of land re-
factors, Mr. Nag examines other
possibilities such a climate and
water, nutrition, health and educa-
tional services etc. in search of an
clear evidence that people in
Kerala use their health facilities
much more than do people in
West Bengal.
.,. form, social equity, education,
\\ women's status, and health care
etc., in Kerala and West Bengal
answer.
Water and Nutrition
Although clim;:ltic conditi()ns are
A major reason for the greater
use of health facilities in rural
Kerala is theil-~
-accessibility,
which have some very similar
features such as high density of
population, traditional emphasis on
not 'Significantly different between
Kerala and West Bengal, Mr. Nag
notes that a safer water supply in
which depends to a considerable
degree on the sm~lIer geographical
area covered by each of them and
education and left-oriented politi- rural Kerala than in West Bengal, on the availability of transport th an
cal activities. However, whereas and the Kerala tradition of drinking in the case of W.J2$Bt engal.
West Bengal has always been more water that has been boiled with Education Fad:Gl'
advanced than Kerala in economic curTrin~eds and the water remain-
Contribution of education to-
development, its mortality level has ing after rice has been boiled may wards better health, not only by
been higher than that of Kerala.
have .contributed ~wald lower imparting knowledge and en-
How is it that Kerala has the morbidity and mortality.
couraging the use of modern health
lowest mortality and fertility levels
Insofar as nutrition is concerned, facilities, but also by inducing
in India while it lags behind the the hypothesis that more effective people to adopt -sound habits of
other States in industrialisation, in- land reforms, the extensive public hygiene and sanitation and to give
come, etc? Dr. Nag poses this distributioo <tffuod "through fair adequate attention to children's
question and then proceeds to price shops, and successful free welfare, has been found to be
find an answer through his analysis school feeding programmes in
(Continued on page 7)
|
|
4 Page 4 |
▲back to top |
New Thinking on Controlling Rural-to-Urban
Migration in Asian Countries
Three Indian mega-cities, viz.,
Calcutta, Bombay and Delhi will
enjoy the dubious distinction of
being among the 14 largest
urban agglomerations in Asia at
the turn of the century. Of these,
Delhi will be registering the second
highest growth rate of 3.72 percent
- equal to that of Bangkok but
lower than Karachi's 3.86 percent
- during the 1990-2000 decade.
In absolute numbers, Calcutta
and Bombay with respective popu-
lations of 16.53 million and 16
million will occupy second and
third positions after Tokyo (popu-
lation 20.22 million) in the year
2000 A.D. in the region comprising
countries of Asia and the Pacific
with a total population of 2.7
billion - 56 percent of the world's
population.
15-Year Pattern of
Urban Growth
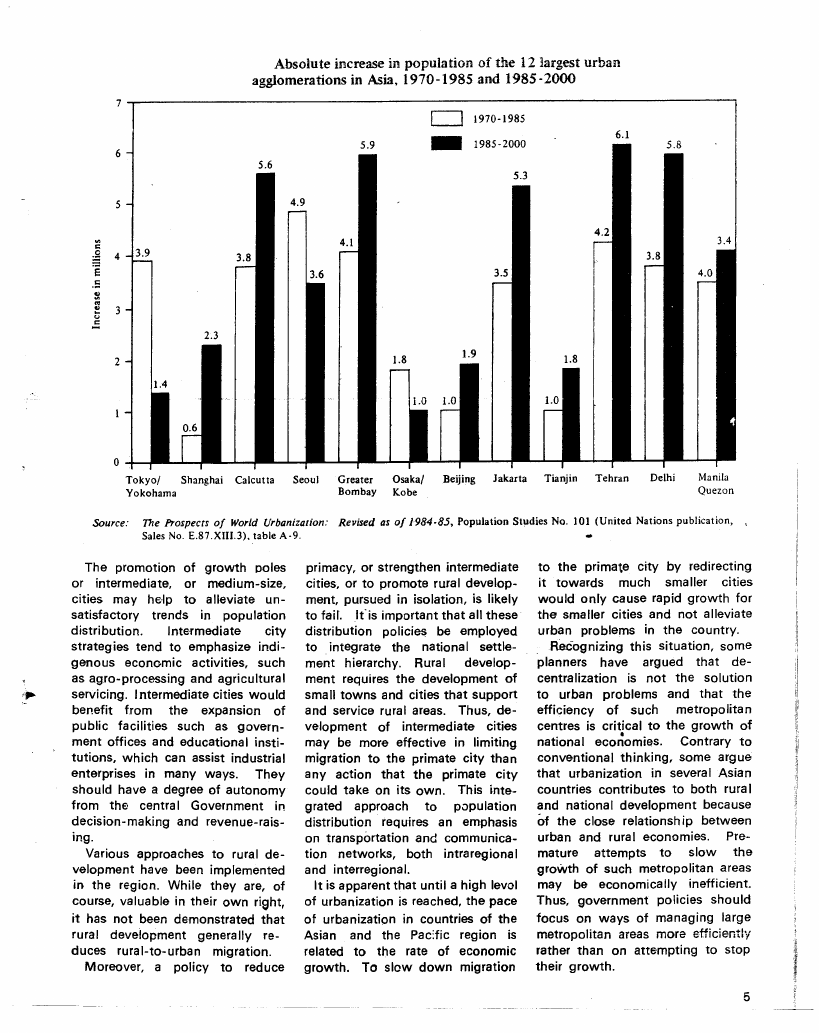
If the absolute increase of the
population of urban agglomera-
tions in Asia in 1970-85 and 1985-
2000 is examined, three distinct
groups emerge.
The first group is composed of
the only three agglomerations in
which the increase in population
during the later period will be
less than in the earlier period,
namely, Tokyo/Yokohama, Seoul
and Osaka/Kobe.
The three Chinese cities of
Shanghai, Beijing and Tianjin com-
prise the second group, in which
the absolute increase during 1970-
85 was 1 million or less but will
increase considerably during the
period 1985-2000.
Calcutta, Greater Bombay,
Jakarta, Teheran, Delhi and Manila/
Quezon city comprise the third
group, in which large absolute
increases occurred during the
period 1970-1985, but in which
the increments during 1985-2000
will be even greater.
.
These revealing though disturb-
ing facts have been brought out in
the Population Research Leads tion, this aspect of urban growth
(pamphlet No. 28 of 1988) pub- has many important social and
lished by the Population Division economic consequences that are
of the U.N.'s Economic and Social of interest to policy makers and
Commission for Asia and the Pacific planners. For instance, internal
(ESCAP) with a view to demons- migration clearly has an important
trating to policy makers and impact on the urban labour force
planners of countries of the Region in some countries where it has
the importance of population distri- permitted the rapid growth and
bution as an integral part of the restructuring of the economy.
development process.
.
A range of policies adopted by a
The Urbanisation Paradox
number of countries in the Asian
There is, however, a mitigating and Pacific region include rural
factor too. In spite of the rapid development strategies, rural re-
increase of the urban population settlement projects, tl)e promotion
in the region over the past quarter of regional growth poles (centres),
of a century, the level of urbanisa- industrial relocation and the build-
tion, o.r the percentage of the total ing of satellite cities.
population living in urban areas, The most common policies have
has increased only gradually. The attempted to slow migration to
percentage urban in Asia in 1960 the largest city or metropolitan
was about 21 (India, 18) and in area of a country, often referred to
1985, about 27 (India, 25.5).
as the "primate city". However,
The paradox of a rapidly increas- these policies have generally not
ing urban population but a simul- been successful. Direct controls
taneous slow rise in the percentage on residential mobility have usually
urban results first, from the level of failee as people find ways to cir-
urbanisation being relatively low, cumvent them.
so that a large proportionaI increase However, even if such policies
does not translate into a great can be successfully implemented,
absolute increase in the level. More it is not clear that they should be.
importantly, however, because rural In many countries, the primate city
population growth rates have re- is the engine of economic growth,
mained high in most countries of and slowing its growth may be
the region until recently, some- harmful to the national economy.
what higher urban growth rates Even when investments in other
have caused only small shifts in areas cost less, they may not be
population towards the urban more efficient. As there is evi-
sector.
dence tha.t primate-city growth
Overall urbanization is of less eventually slows down spontane-
concern to planners and policy ously, it is not certain that early
makers than population size and intervention to accelerate the pro-
growth in individual urban areas. cess is desirable. It is important,
It is the later aspects that pose therefore, that policy be formulated
severe challenges in the region as on a country-by-country basis.
many of the world's largest cities
Policies that may be more
are and will be in Asia. For exam- . successful are politically difficult
ple, the population of Tokyo/ to implement. These would in-
Yokohama will exceed 20 million clude eliminating indirect spatial
by the end of the century.
policies that have a primate-city
Because the expansion of the bias, allocating more funds for
large cities in the region occurs to infrastructure to other cities, and
a significant degree due to migra- industrial relocation.
|
|
5 Page 5 |
▲back to top |
5
c'"::
~ 4 3.9
'5
.5
~:•.•l
.u.:
3
2
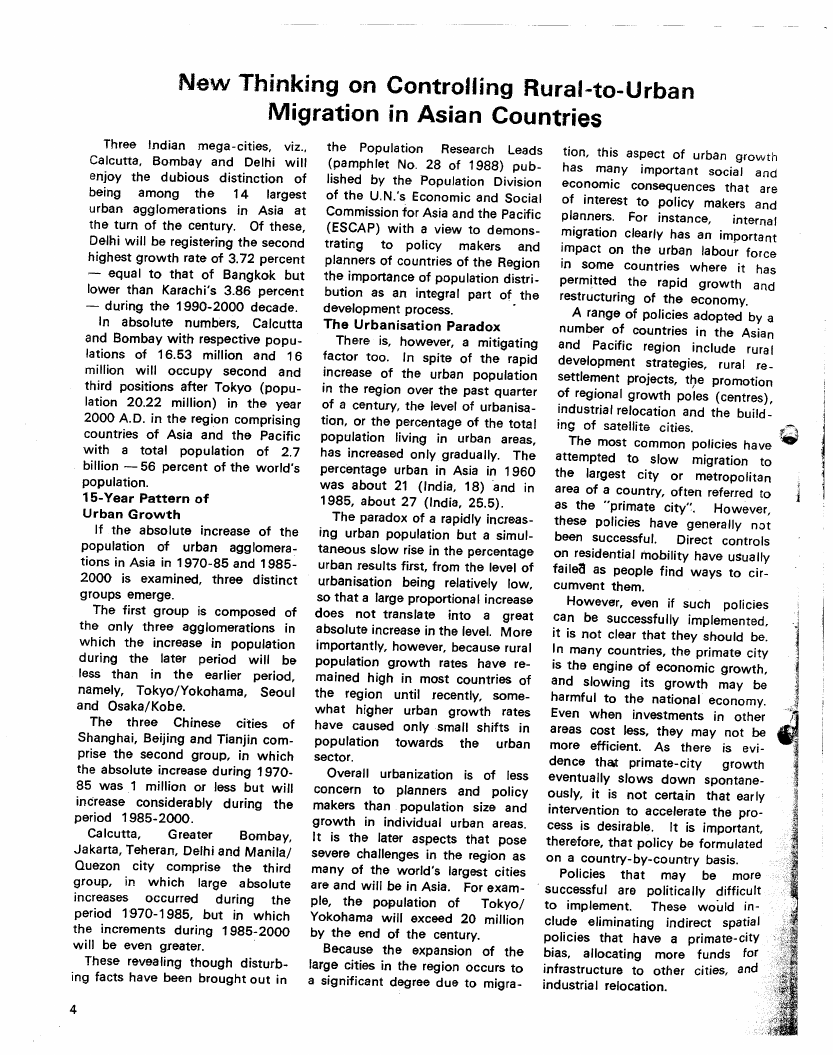
Absolute increase in population of the 12 largest urban
agglomerations in Asia, 1970-1985 and 1985 -2000
c=J 1970-1985
11III 1985·2000
Tokyo/ Shanghai Calcutta
Yokohama
Seoul
Greater Osaka/
Bombay Kobe
Beijing Jakarta
Tianjin
Tehran
Delhi
Manila
Quezon
Source: The Prospects of World Urbanization: Revised as of 1984·85, Population Studies No. 101 (United Nations publication, ,
Sales No. E.87.XIII.3), table A -9.
••
The promotion of growth poles
or intermediate, or medium-size,
cities may help to alleviate un-
satisfactory trends in population
distribution.
Intermediate city
strategies tend to emphasize indi-
genous economic activities, such
as agro-processing and agricultural
servicing. Intermediate cities would
benefit from the expansion of
public facilities such as govern-
ment offices and educational insti-
tutions, which can assist industrial
enterprises in many ways. They
should have a degree of autonomy
from the central Government in
decision-making and revenue-rais-
ing.
Various approaches to rural de-
velopment have been implemented
in the region. While they are, of
course, valuable in their own riaht,
it has not been de·monstrated that
rural development generally re-
duces rural-to-urban migration.
Moreover, a policy to reduce
primacy, or strengthen intermediate
cities, or to promote rural develop-
ment, pursued in isolation, is likely
to faiLlfis important that all these
distribution policies be employed
to integrate the national settle-
ment hierarchy. Rural develop-
ment requires the development of
small towns and cities that support
and service rural areas. Thus, de-
velopment of intermediate cities
may be more effective in limiting
migration to the primate city than
any action that the primate city
could take on its own. This inte-
grated approach to p.:>pulation
distribution requires an emphasis
on transportation and communica-
tion networks, both intraregional
and interregional.
It is apparent that until a high level
of urbanization is reached, the pace
of urbanization in countries of the
Asian and the Padic region is
related to the rate of economic
growth. To slew down migration
to the primate city by redirecting
it towards much smaller cities
would only cause rapid growth for
the smaller cities and not alleviate
urban problems in the country.
Recognizing this situation, some
planners have argued that de-
centralization is not the solution
to urban problems and that the
efficiency of such metropolitan
centres
national
iseccorinti•coaml ietso.
the growth
Contrary
of
to
conventional thinking, some argue
that urbanization in several Asian
countries contributes to both rura I
and national development because
of the close relationship between
urban and rural economies. Pre-
mature attempts to slow the
growth of such metropolitan areas
may be economically inefficient.
Thus, government policies should
focus on ways of managing large
metropolitan areas more efficiently
rather than on attempting to stop
their growth.
|
|
6 Page 6 |
▲back to top |
F.P.f. to organise Regional Workshops and
National Seminar
With the active cooperation of sures to promote family planning
various Chambers of Commerce acceptance in the industrial sector.
and Industry, the Family Planning The national seminar to be held
Foundation-has planned a series of at New Delhi will focus attention
nine regional workshops and a on the policy measures required
national s€·minar in its calendar of to be adopted at the national level
activities for 1989.
in the light of the recommenda-
The programme has twin objec- tions of the regional workshops.
tives: to create a powerful con- The entire programme is expected
sensus on the role of the organised to go a long way in reaJising the
sector, more particularly the private long-term goal of sensitising the
sector, in providing enlightened Indian industrial leadership and
leadership to tackle the country's managements about the serious-
most baffling problem, viz., un- nesS of the problem of population
hindered population growth, and growth and the need to check it
to evolve suitable strategies for with a sense of urgency and
establishig employment-based self- resoluteness.
sustaining family welfare services.
After the conclusion of the pro-
The regional workshops are to gramme, the Foundation intends
be organised at Ahmedabad, to develop a manual and a set of
Bangalore, Bhopal, Bombay, guidelines on how to start volun-
Calcutta, Chandigarh, Kanpur, tary family welfare activities in
Madras and Ranchi. In these industrial enterprises and to moni-
workshops employers and mana- tor their performance. These will
gers, workers and trade unionists, be distributed to Chambers of
social workers and representatives Commerce and Industry and asso-
of programme implementing agen- ciations of industries all over the
cies will discuss and devise mea- country.
Project to Harness Youth
Power for Population Control
On November 14 this year, the
Nehru Yuva Kendra (NYK) Sanga-
than and the Family Planning
Foundation will be celebrating the
birthday Of Pandit Jawaharlal Nehru
by launching a project intended to
harness the youth power of the
nation in the all-important cause
of population control.
A start is being made on this
collaborative motivation and re-
orientation training project to be
implemented through the N.Y.K.
network, with four northern states,
viz., U.P., Bihar, Rajasthan and
M.P., which incidentally have
shown poor performance in the
implementation of family planning
programme.
Initially, 150 District Coordina-
tors in these States will be given
thorough reorientation vis~a-vis
dynamics of population growth
and its dangerous implications to
the well-being of the individual
and the nation, as also how to
undertake awareness and motiva-
tion campaigns. Having been
equipped with the necessary skills
and audio-visual and other com-
munication aids, these district co-
ordinators will take the messageof
small family norm to the youth
leaders operating at the village
level who in turn will be trained
and equipped to involve rural
youth and communities for pro-
moting family welfare activities.
Women attending the craft centres
being run under the N.Y.K. set-up
will also be imparted family life
education under this project.
Initially, the project is for 18
months with the possib!lity of
continuing for another 18 months.
Video Films for Promo-
ting Health and Family
Welfare Activities
The Family Planning Foundation
has produced four video films as a
part of its efforts in promoting a
deeper appreciation of the socio-
cultural dynamics of family welfare
programmes. The films and their
themes are:
1. "Too Early, Too Many, Too
Soon" -
The film makes an indepth
humanistic study of the crucial
issue of high infant mortality
prevailing under diverse socio-
economic conditions. It is a
powerful plea for mitigation of
circumstances responsible for
this sad state of affairs.
2. "How They Left Hell
Behind" -
It highlights the efforts of
the Working Women's Forum,
Madras in bringing about
social transformation in th.e
life.,.of the poorest women
living in the slums of Madras
and else'!Vherethrough com-
munity-based action. The
film has an in-built family
welfare appeal.
3. "Triumph Qver Rock" -
This film depicts the uni-
que efforts of the renowned
Arole couple - the Magsaysay
Award winner Dr. Raj Arole
and his equally dedicated wife
Dr. MabeLArole - in building
up at Jamkhed village of
Maharashtra an indigenous
health and family infrastruc-
ture with the fullest participa-
tionof the community at
large.
4. "Planting a New Way of life"-
The film shows how the
plantation workers in the NiI-
giris have been intimately
involved in promoting a
scheme aimed at propagat-
ing the small family norm
within the larger framework
of family welfare.
|
|
7 Page 7 |
▲back to top |
Promoting FamilyP'ann~ng Among
Industrial Workers
low Mortality in KeraJa
(Continued from page 3)
On July 11, 1987 when the force, 6,830 couples, i.e., 40.16
world population crossed the five per cent constituted the target
billion mark, the Family Planning couple group.
Foundation initiated a two-year
In order to motivate the workers
tripartite project of far-reaching im- and the management as also the
port in so far as the acceptance of official agencies like the ESIC and
small family norm by workers in State Medical Department, four
the organised sector is concerned. workshops/group meetings were
The project expected to serve as organised in different industrial
a model of cooperation between zones of Gurgaon and adjoining
employers, employees and institu- villages. Two family welfare coun-
tions providing family welfare selling centres have been opened
services covers small, medium and with the assistance of the indus-
large industrial units of Gurgaon tries and the local medical authori-
and Faridabad in Haryana, and ties and the ESIC. These centres
Okhla in Delhi. It is run by two provide population education,
voluntary agencies having con- family life education to the workers
siderable experience of family wel- and their families and also make
fare work.
available contraceptives to 'the tar-
While the family welfare Founda- get couples.
tion of the Punjab, Haryana and
With persistent pursuasion it has
Delhi Chambers of Commerce has been possible to secure the in-
been entrusted with the task of volvement on a long-term basis of
executing the project for industrial 23 industries. These industrial
units located at Gurgaon and units will maintain the eligible
Faridabad, Parivar Seva Sanstha couple registers to be updated
looks after the Okhla industrial from time to time.
units.
The five immunisation camps
During the first year of imple- ..proved very popular and in these
mentation, the project has shown camps 700 children were immunis-
very encouraging results in generat- ed against polio, tetanus, dip-
ing awareness among industrial theria, whooping cough, TB and
workers and managements .Ieading measles.
to increased demand for family
In the five worker motivator
welfare services. Here we take training camps organised in diffe-
note of the achievements of the rent industries, 122 workers were
Gurgaon chapter.
trained. These worker motivators
Starting with the baseline survey, will be of great help in disseminat-
organisation of workshops, group . ing the message of small family
meetings, preparation and mainte- norm among the fellow workers.
nance of Eligible Couple Registers Out of these 11 worker motivators
(ECR), opening of counselling have been selected for active in-
centres and holding of immunisa- volvement and will be paid an
tion camps bave been the main honorarium of Rs. 100/ - p.m.,
activities at Gurgaon.
from July 1988. Their performance
The baseline survey revealed that will be evaluated every month.
out of 600 industries contacted,
Apart from creating a general
572, i.e., 95.3 per cent employed climate for adoption of small family
a work force of less than 100. Out norm as a way of life, these activi-
of a total number of 16,980 workers ties have resulted in 98 persons
employed in these industrial units, undergoing sterilisation, 40 women
1 S, 157, Le., 95.15 per cent were accepting Cu-T and 275 persons
male workers and only 823 female ta king to conventionaI contra-
workers. Among the total work ceptive.
quite significant. Rural education,
women's education and primary
education are especially important
in the fight to reduce mortality rates.
In 1971, 76 per cent of Kerala's
urban population aged five years
and above were literate, compared
with 62 per cent in West Bengal.
For the rural populations the corres-
ponding figures were 69 per cent
and 31 per cent. In the same year,
61 per cent of Kerala's rural females
were literate, compared with 18
per cent in West Bengal. In 1981,
74 per cent of children in the age
group 5-9 years in rural Kerala
were enrolled in primary schools,
whereas this figure in West Bengal
was onIy 32 per cent.
Analysing the educational struc-
ture in the two States in order to
understand the factors responsible
for more equitable distribution of
educational services in Kerala, Mr.
Nag notes that while in Kerala
there was emphasis on primary
education in Malayalam, there was
strong advocacy of secondary edu-
cation in the English language in
urban areas iR West Bengal rather
than primary education in rural
areas.
The resources allocated to educa-
tion have always been greater in
Kerala than in West Bengal. The
proportions of expenditure on diffe-
rent sectors of education in the
two states reflect their different
priorities. Thus in 196'9-70, 59
per cent of .Kerala's educational
funds were spent on primary educa-
tion, compared with 38 per cent in
West Bengal. In the same year,
the proportions going to university
were 5 per cent and 16 per cent
respectively. During the 19805 the
priorities in West Bengal have
changed considerably in favour of
greater equity in educational ser-
vices, but atleast up to the end of
the 19705, these were more equit-
able in Kerala - an important
factor contributing to the lower
mortality in this state.
|
|
8 Page 8 |
▲back to top |
Main Suggestions &
Recommendations
of the Seminar
Dr. Harcharan Singh
Adviser Planning
Commission chaired
the Seminar on
i. High risk mothers should be
identified on the basis of
maternal and social-economic
factors in order to provide
. nutrition and health support
to them on a priority basis..
ii. Contraceptive counselling and
services should be made avail-
July 2. On his
right Dr. Susanne
Mowat of I.D.R.C.
and on his left
Mr. Harish Khanna
Executive Director
FP.F. .
also to ensure the quality and
Pleading for a humane approach
able to women both at pre-
equity of health and family instead of a purely statistica I
conception and post-partum
welfare services.
approach, Prof. P. C. Joshi, from
stages to break the vicious viii. Appropriate medica.l and Institute of Economic Growth, em-
circle of high infant mortality,
social interventions should be phasised the need for interaction
and high fertility, particularly
tried and experimented on a with people, probing into their
among the poorer sections of
society.
pilot basis ta arrive at a minds and situations and con-
proper mix of feasible and ducting of in-depth case studies
iii. "At-risk" infants should be
replicable interventions in for collecting qualitative data to
identified on the basis of
different population groups. understand and solve the problem
low-birth weight, poor health ix. The risk factors should be of high infant mortality and ferti-
and nutrition status and
prioritized carefully and appro- lity.
growth faultering with a view
priate interventions recom-
to providing needed health
mended selectively in view of Report Presentation
care and attention and moni-
financial constraints.
The main findings of the State-
toring their progress on a x. The findings should be made wise studies were presente'd by
priority basis.
available to public as well as Project Leaders: (i) Dr. M. S.
iv. Primary health care system
policy makers in simple terms Ashraf for hilly and rural areas of
should be restructured and
and regional languages to in- Uttar Pradesh, (ii) Dr. Rita Sapru
revitalized to provide nece-
crease their awareness about for rural and tribal areas'of M.P.,
ssary health and family wel-
risk factors and risk-modify- (iii) Dr. Nityanand Patnaik for
fare services in an integrated
ing interventions.
tribal ,areasof Orissa, (iv) Dr. P. H.
manner to the needy at the
Agenda for Action
Reddy for rural and urban areas of'
right time, particularly, during
the natal and per-natal stages.
(Continued from Page 2)
Karnataka, and (v) Dr. Victor S.
D'Souza for Bombay slums. After
v. ANMs, health guides and Dais tion of all the recommendations these state-wise presentations, the
should be trained and re- made by the Task Force on the consolidated report was presented
trained in simpler and appro- minimum peri-natal care.
by Dr. B. R. Patil, Project Director,
priate medical and social inter-
ventions to accelerate the rate Motivate Grass-root Workers
FPF, as overall project incharge.
Dr. R. S. Arole, Director,
of reduction in both infant
Dr. Harcharan Singh, Adviser, Society for Comprehensive Rural.
mortality and fertility as a lot Planning Commission, admitted Health Project in India, Jamkhed,
depends on them and their that the existing health care system said tf"lat in spite of poverty a lot
efforts.
was not properly and adequately could be done to reduce infant
vi. Mothers should be made geared to avert the infant deaths, mortality by educating grass-root
aware of risk factors and risk 60 percent of which took place health workers and the community
moderating
interventions within one month from birth. He itself on simple hygienic practices
through appropriate informa- said that without the needed quali- and dietary intakes. If the quality
tion, education and com- ty of services and commitment of of services and credibility of pri-
munication strategies, and health personnel it would not be mary health care system could be
also enabled to take care of possible to achieve' the desired improved, the targets could be
their health.
results in spite of their having achieved in much shorter time
vii. Community participation and built up a vast health care system. even under the existing system.
involvement of local organisa- In this context, he emphasised the
The seminar concluded with a .
tions should be encouraged to need for motivation, training and summing-up of various view-points
the extent possible not only education of grass-root health expressedduring the two-day dell'
to generate demand for but functionaries.
berations, by Dr. Pati!.
Published by the Family Planning Foundation, 198 Golf Links, New Delhi 110003. Tel: 62(~ 35'060907158631. 9278
Printed at the Statesman Press, The Statesman Ltd., Connaught Circus, New Deihl 11 •