





 |
Focus 1989 April - June |
|
|
1 Page 1 |
▲back to top |
ICMR Study Focuses on .
Poor Quality of Maternal & Child Health and Family
Planning Services at Grass-roots Level
At the second meeting of the Central Council for Health and Family
Welfare held at New Delhi from February 1 to 3, 1989, Dr. Badri Saxena
of the Indian Council of Medical Research (lCMR) presented the findings
of a significant study on the quality of maternal and child health (MCH)
and family planning services at the Primary Health Centres (PHCs).
Conducted through a network of 33 Human Reproduction Research
Centres (HRRCs) attached to medical colleges, between May 1987
and April 1988, the study covering 99 districts and 198 Primary Health
Centres in various States of the country, presents a grim picture of health
care and family planning services at the grassroots level with all-round
inadequaciesof personnel, their training, availability of drugs and contra-
ceptives, equipment and other supportive facilities, outreach and
coverage, etc.
'This revealing though disturbing
study merits much wider attention
in the interest of achieving the
goals set under the national health
and family welfare programmes.
We present below the salient
features of the study.
Primary Health Centres:
Many Gaps
The recommended pattern of a
PHC for 30,000 population was
achieved by only 15 per cent of the
PHCs. The State of Maharashtra
was found to be largely imple-
menting the recommended pattern,
whereas the States of U.P., West
Bengal, Rajasthan and Haryana
were far behind with PHCs cover-
ing by and large a population of
more than 1,20,000. More than half
of the 'remote' villages were located
at a distance of 5 kms. or more
from the nearest health facility
and this could be one of the major
reasons for the poor outreach and
coverage of family welfare services
as well as its under utilisation.
Availability of Resources:
Major Deficiencies
(i) Manpower: The major defi-
ciency in manpower was in
regard to the availability of
Auxiliary Nurse Midwives
(ANMs); only 15 per cent of
the PHCs fulfilled the recom-
mended norm of one ANM
per 5000 population. Though
the position about Medical
Officers was relatively better,
there was, however, defi-
ciency regarding the avail-
ability of Lady Health Visitors
(LHVs) who were supervIsing
in most instances 5 to 10
ANMs against the recom-
mended norm of 4 ANMs.
(ii) Supply of medicines and
contraceptives: By and large,
all categories of general medi-
cines were not available in
optimal amounts and anti-
biotics were in short supply.
Amongst emergency drugs,
the' most disturbing feature
was absence or inadequate
supply of oxygen as well as
Corticosteroids
a life-
saving drug. The supply posi-
tion of vaccines and contra-
ceptives was satisfactory.
(iii) Equipment and Facilities: The
major deficiency noted was
regarding labour rooms and
operation theatres, which were
either absen\\ or not equipped
properly in majority of in-
stances. Maintenance of cold
chain equipment continues to
pose a major problem.
Quality of Services:
Uniformly Poor
, °With regard to ante- natal care,
per cent of PHCs did not have
any records of pregnant women;
50 per cent were registering 40
per cent of pregnant women and
only 11 per cent were registering
|
|
2 Page 2 |
▲back to top |
80 per cent of the pregnant women.
The situation was equally dismal
vis-a-vis completecoveragG by two
doses of tetanus toxoid and iron-
folic acid administration - only
about 13 per cent of PHCs were
covering 60 per cent or more of
pregnant women with full dose of
tetanus toxoid while only 11 per
cent PHCs were administering
iron-folic acid to more than 60
per cent pregnant women.
The majority of the sub-centres
had no facilities for routine check-
up of pregnant women or for
weight and blood pressure record-
ing, estimation of haemoglobin or
urine examination. Majority of
ANMs rendering intranatal care
did not use the sterilised delivery
kits and several procedures carried
out by them such as cord cutting,
perineal care and resuscitation of
the new-born were grossly un-
satisfactory. Most probably this
indicated lack of emphasis on these
asp3cts in the training of ANMs.
The quality of post-natal care
delivered by the AN Ms was also
found to be uniformly poor. Neo-
natal care was limited to mostly
giving advice on care of the cord
and feeding practices. None of the
PHCs were maintaining systematic
records relating to infant or mater-
nal deaths. Birth weights were not
taken, and if taken were not entered
in the records.
Outreach of Family
Type of Village
Total number
of villages
covered
P.H.C.
SUB-CENTRE
REMOTE
193
585
1130
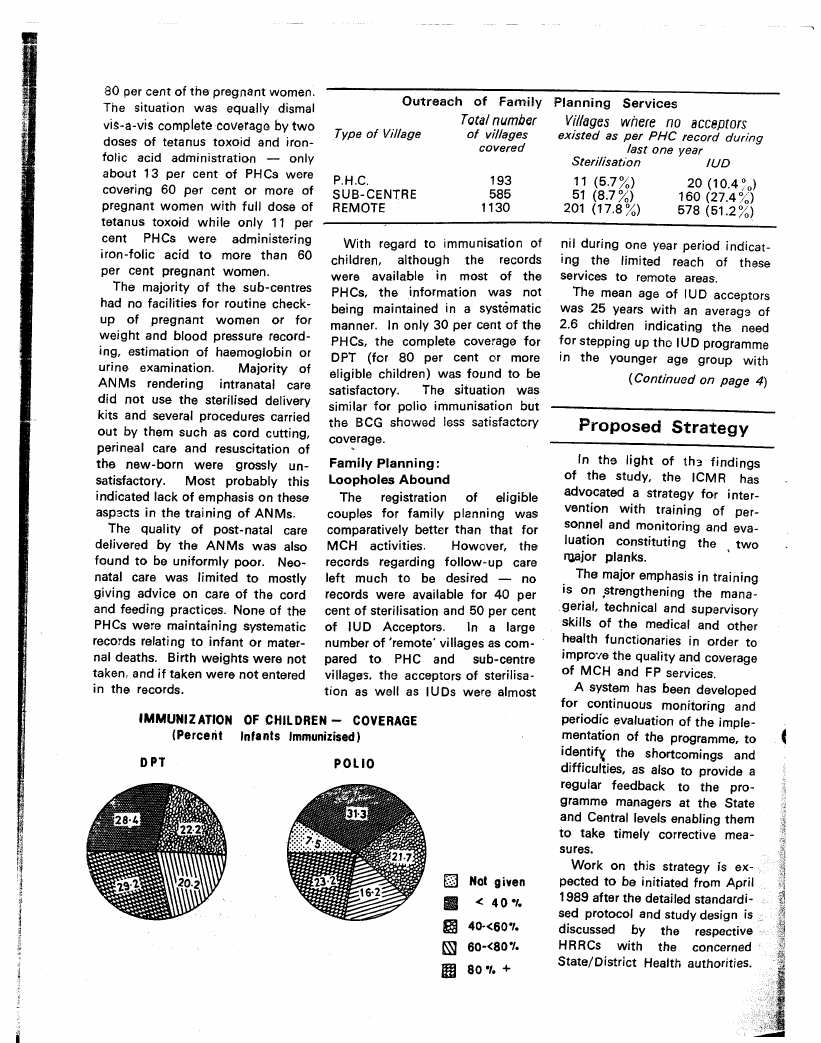
With regard to immunisation of
children, although the records
were available in most of the
PHCs, the information was not
being maintained in a systematic
manner. In only 30 per cent of the
PHCs, the complete coverage for
OPT (for 80 per cent or more
eligible children) was found to be
satisfactory. The situation was
similar for polio immunisation but
the BCG showed less satisfactory
coverage.
Family Planning:
Loopholes Abound
The registration of eligible
couples for family planning was
comparatively bettN than that for
MCH activities. Howover, the
records regarding follow·up care
left much to be desired - no
records were available for 40 per
cent of sterilisation and 50 per cent
of IUD Acceptors. In a large
number of 'remote' villages as com-
pared to PHC and sub-centre
villages. the acceptors of sterilisa-
tion as well as IUDs were almost
IMMUNIZATION OF CHILDREN - COVERAGE
(Percent Infants Immunizised)
Not given
< 40·,.
40-<60·'.
60-<80·'.
Planning Services
Villages where no acceptors
existed as per PHC record during
last one year
Sterffisa&on
IUD
11 (5.7 %)
51 (8.7 %)
201 (17.8 %)
20 (10.4 ~o)
160 (27.4 %)
578 (51.2 %)
nil during one year period indicat-
ing the limited reach of these
services to remote areas.
The mean age of IUD acceptors
was 25 years with an averaga of
2.6 children indicating the need
for stepping up tho IUD programme
in the younger age group with
(Continued on page 4)
Proposed Strategy
In the light of th3 findings
of the study, the ICMR has
advocated a strategy for inter-
vention with training of per-
sonnel and monitoring and eva-
luation constituting the two
ruajor planks.
'
The major emphasis in training
is on ,strengthening the mana-
gerial, technical and supervisory
skills of the medical and other
health functionaries in order to
improve the quality and coverage
of MCH and FP services.
A system has been developed
for continuous monitoring and
periodic evaluation of the imple-
mentation of the programme, to
identifx the shortcomings and
difficulties, as also to provide a
regular feedback to the pro-
gramme managers at the State
and Central levels enabling them
to take timely corrective mea-
sures.
Work on this strategy is ex-
pected to be initiated from April
1989 after the detailed standardi-
sed protocol and study design is
discussed by the respective
HRRCs with the concerned
State/District Health authorities.
|
|
3 Page 3 |
▲back to top |
Make Famiily Planning Broad-based P,eopJe's Movement
Minister's Call at Central Council for
Health & Family Welfare Meeting
Ms. Saroj Khaparde, Union
Minister of State for Health and
Family Welfare, in her inaugural
address at the recent three-day
meeting of the Central Council for
Health and Family Welfare, spoke
of thQ need for making family
planning a people's movement and
for greater decentralisation of
health planning and family wel-
fare programmes.
She pointed out that the target
of reducing population growth rate
to 1.9 per cent, by the Seventh
Plan, was not likely to be achieved.
This could be because the family
welfare programme was not as
broad-bas3d as it should have
been. She said that the State
governments had been given en-
hanced powers to sanction upto
Rs. 10 lakhs a year for any project
sponsored by a voluntary agency.
She asked them to make greater
use of these powers and involve
greater number of voluntary
organisations in family welfare pro-
grammes.
Noting the serious shonfalls in
the establishment of primary health
centres and sub-centres, she urged tives/awards. These should be
upon the States and Union terri- community based and related not
tories whose performance was only to family planning but to the
below target to make special efforts pe for.nance of other health and
to set up or operationalise these development activities, relevant to
centres.
fertility decline, like MCH, immu-
More Resources Needed
nisation, female literacy and nutri-
Mr. R. Srinivasan, Secretary, . tion, he said.
Ministry of Health and Family
Welfare, in his welcome speech,
called for more resourcesfor health
and family welfare projects. 'What-
ever be our strategy or priorities, it
is plain that additional resources
are required to make any effective
impact on the health scene', he
said, pointing out that the share
of the health and family welfare
sector in the Seventh Plan was
only 3.7 per cent of the total
allocation.
Improve Programme
Management
Mr. P. N. Srivastava, Member,
Planning Commission, pointed out
that health and family plann:ng
programmes in India suffered from
lack of support, supervision and
poor management. He said that
high priority should be given for
training of health personnel as
public health managers.
Pleading for optimal uSe of the
huge infrastructure of primary
health centres, community health
centres and sub-centres through
provision of essential inputs and
staff, he said that the effectiveness
of health centres would remain
limited if they were not integrated
with other health-related services
like nutrition, safe drinking water,
education, information and com-
munication.
Mr. Srivastava also suggested
rationalisation of existing incen-
Thrust of the
Recommen'dations
While making significant recom-
mendations for attainment of the
demographic goals, the Central
Council of Health and Family Wel-
fare has emphasized the need for
adoption of a mix of "before and
beyond contraception" strategies,
alongside a geClring up of the
contraception promotion and deli-
very system. The strategy should
focus on bringing down growth
rate, recruiting younger people as
acceptors of small family norm
and enhancing the effectiveness of
child survival and maternal health
programmes.
The recommendations aim at
strengthening the thrust of the
(Continued on page 7)
|
|
4 Page 4 |
▲back to top |
Nutritional Health of Children'
A New Dimension
JCM R Study Findings
(Continued from page 2)
Once seen mainly as a problem months, about the need to feed 5 lower parity to achieve the nece-
of production, then as a prob- small child twice as often as an ssary demographic impact. One of
lem of distribution, then as adult, about the need to enrich the the major drawbacks noted in this
of 'en~itlemenf, it is time to add family's ordinary food with a little regard was that one third of the
one further layer to the .under- oil or fat, about tho need to give a AN Ms did not have any idea
standi ng of the nutrition problem child small amqunts of green about the availability of the stock
and its potential solutions.
vegetables each day, about the of Nirodh and oral pills with them.
Both in scale and in severity, it is need to continue giving food and l'his could affect the credibility of
the child who is most affected by fluids during illness, about the AN IYJswith the potential acceptors
malnutrition. By the age of five, need to pay special attention to of these methods.
most of the growth of the child's feeding in the week after an illness
The mean age of sterilisation
brain and body is complete. There so that the child can 'catch up' on acceptors was 29 years with mean
is no second chance. And if en- the growth lost, and about the parity of 3.6. In view of its accep-
hancing human capacity is the need to regularly check that a child tance by high parity women, the
aim and the measure of real de- is gaining we:ght from one month efficacy of the sterilisation method
velopment, then there is no greater to the next.
as a sheet anchor of the family
priority than maintaining the nutri-
In addition to all of these factors, planni ng programme is rather
tional health of children in these poor nutritional health in preg- doubtful.
vital years.
nancy can lead not only to low
l'he study also evaluated the
But it has become clear in the birth weight but also to the mal- quality of sterilisation services -
last decade that lack of food in the nutrition of the child in its early pre-operative, operative and post-
home is not usually the main cause years. Maternal health, and the operative - offered through camps.
of child malnutrition.
spacing of births at least two years In all 132 camps were assessedby
Paradoxical as this may seem to apart, are therefore also major HRRCs teams. In general, the
a public accustomed to the idea factors in child nutrition. "In the facilities at the camp sites were
that food shortages, hunger, and past", says Edgar Mohs a Iformer sat~actory with regard to t'aking
malnutrition are virtually synony- Director of the National Children's prior consent, ensuring privacy and
mous, the fact is that a combination Hospital and present Minister of conducting the procedures with
of other factors have an even Health in Costa Rica, "We believed pre-medication and under local
greater influence on [nutritional that the lack of food was a major anaesthesia. However, glaring defi-
status. In particular, illness is cause of illness and malnutrition. ciencies were noticed vis-a-vis
known to depress the appetite, We have now started to accept availability of transport and life
reduce the absorption of food, that family spacing, breast-feed- saving drugs in case of any emer-
drain away nutrients in diarrhoea, ing and the control of infectious gency. Screening for detection
and burn up calories in fever. And diseaseare the keys to eradication." of anaemia, hypertension and dia-
the sheer frequency of nutri- (From UNICEF's State of World's betes was not carried out routinely
tionally debilitating illnesses among
Children Report 1989)
for all women. Further, in such
children in poor communities is
one of the major causes of poor
growth.
Of possibly equal importance is
the fact that most parents have
Studies on new Male
Contraceptive
Scientistsat the National Institute
of Nutrition (NIN) have found mahua
oi~is not only edible, but has a rever-
camp situations, sterilisation was
never deferred or refused to a
potential acceptor even when the
physical condition of the women
. warranted this. In more than 33
not been empowered with today's
knowledge about the special nutri-
tional needs of the very young
child - knowledge about the
importance of breast-feeding,
sible contraceptive effect on males.
Male rats fed on mahua oil
becameinfertile, according to the NIN
study. Fertility was restored once the
rats were taken off the oil diet for
three weeks. Studies are yet to be
per cent of .the camps, the equip-
ments/instruments used for surgery
were either not sterilised at all or
improperly sterilised, and in more
than one third of the subjects the
about the need to begin adding
repeated in humans.
abdominal and perineal parts were
other foods at the age of 4 to 6
not prepared properly for operation.
I
LIi
|
|
5 Page 5 |
▲back to top |
Why Non-terminal Methods are not
so Popular In India?
India is probably the only country
in the world that depended almost
completely on sterilisation to push
forward its fqmily welfare pro-
gramme. The share of non-terminal
methods in the total Couple Pro-
tection Rate (CPR) has been quite
The acceptancG of non-terminal
methods is comparatively higher
among urban dwellers than among
rural dwc:lers mainly because of
the former's bettor,educational level
and exposuro to new ideas includ-
ing fertility regulation. Thesame
marginal - it varied between 2.2
to 3 per cent during the period
1970-1982. It is only since 1983-
84, when the Government of India
decided to lay more emphasis on
popularisation of non -terminal
methods, that some improvement
is discernible. In 1986-87, the
contribution of non-termi nal
methods waS 9.6 per cent out of a
total Couple Protection Rate of
37.5.
In its working paper series (W.P.
89/1, January 1989), Population
Research Centre of JSS Institute of
Economic Research, Dharwad
(Karnataka), the Research Investi-
gator, Mr. J. B. Hasalkar attempts
to investigate the factors inhibit-
ing use of non-terminal methods of
contraception in India based on a
number of existing studies and
research reports.
can be said about the extension of
knowledge regarding different non-
terminal methods. Since the non-
terminal methods require conti-
nuous use, stro,ng motivation in the
form .of psychological prepared-
ness and putting up with certain
side-effects, if they are not of
serious nature, is absolutely essen-
tial. However, the complaints of
menstrual disorders due to USeof
IUD, and oral pill are the most fre-
quently mentioned, causing much
damage to the acceptance of these
methods. Further, pill and con-
dom are considered as most in-
convenient to use.
Important factors from the pro-
gramme supply angle have been
indicated as (i) Excess emphasis
on terminal methods; (ii) lack
of sustained motivation; (iii) pre-
ference for service extension by
qualified personnel; and (iv) inade-
Factors Inhibiting Acceptance
quate IEC activities.
Comparatively lower preference
Right from the inception of the
for non-terminal methods seems to family welfare programme, there
be the cumulative resuits of the has been excess emphasis on
inte~action between the com- terminal methods and the much
munity's demand and programme publicised "cafetaria approach" has
personnel's supply factors. So far been in name only. Since non-
as the community's demand is terminal methods required sus-
concerned, the plausible inhibiting tained motivation, probably they
factors are listed as (i) Lower lite- do not find much favour with the
racy level of the couples; (ii) lack programme personnel due to their
of knowledge about non-terminal target-oriented approach. Exten-
methods; (iii) lack of psychological sion of family planning service by
preparedness to accept; (iv) in- a berter qualified and experienced
fluence of adverse side-effects ex- person and prompt follow-up ser-
perienced by the acceptors and of vice has always ensured higher
rumours about such effects, and acceptance and continuation rates.
(v) use convenience of the method. This perhaps explains much berter
IUD retention rates in urban areas
as compared to rural areas. Fur-
ther, the IEC activities are much
too inadoquate, espocially in the
countryside to leave an effective
impact. The only channel of IEC
activities, that is somewhat effec-
tive i~ tho grass-roots level workers,
while theorient1tio'n training camps
erganised by the PHCs are just
ritualistic, devoid of any tra:ning
component.
Dim Prospects
The working paper concludes,
unless there are drastic, structural
improvements in the community's
living standards, we can not expect
large scale use of non-terminal
methods. Under tho circumstances,
the prospects of populerising the
non·'term~'nalmethods in immediate
future, either through extended em-
phasis or excess emphasis seem
quite bleak in rural areas. A
moderate success, however, can
be expectedln urban areas because
of their comparative advantageous
position. The onry alternative left,'
for the time being at least, is to
continue emphasising sterilisation,
with the changed motivational stra-
tegy making couples to accept it
after two children for real demo-
graphic impact.
Caretakers of Trees
"Had women been caretakers
of trees, more forests might still
be intact. 'To a rural woman in
India... forests are a sustainable
source of fuelwood and fodder,
materials she now expends more
than twice as much time collect-
ing than she devotes to agri-
culture." From the Forgotten
Resource in Worldwatch.
(World Development Forum,
No. 19, Vol. 6, 1988)
|
|
6 Page 6 |
▲back to top |
Human Survival Concerns
-
In pursuance of its decision to
bas'3 all its youth leade~ship train-
ing progammes in the year 1989-
90, conth') theme of Human Sur-
vival Values, the Nehru Yuva
Kendra Sangathan (NYKS), con-
ducted a programme 'Training for
'Trainers', at the Commonwealth
Youth Programme; Asia Centre,
Chandigarh from January 31 to
Fo'::-ruary8, 1989.
This in-house training programme
was attended by 17 Regional
Co::>rdinatorsand two Youth Co-
ordinators of the Sangathan. Drawn
from various regions of the coun-
try, their area of operation extends
to some 200 districts covering nine
lakh youths in nearly 30,000
village youth clubs.
Mr. Vikram Diesh, Director Train-
i ng & Evaluation of NYKS, told
'Focus' that the:r Youth Leadership
Training Programme was aimed at
training a cadre of dedicated Youth
workers who would become cata-
NYKS
Training
Programme
at
Chandigarh
Iysts of socio-economic change
with the ultimate objective of im-
proving the quality of life of the
rural youth.
The Family Planning Foundation
;s funding the first phase of this
training project to the tune of
Rs. 5 lakhs which will be mainly
utilised for producing a package,of
comm\\;lnication/training materials
suitable for different regions of
the country.,
Population Major Cause of Deforestation in India
India may have already gone
beyond the threshold of tolerable
levels in the loss of its forests,
Mr. Attila Karaosmanoglu, the
World Bank Vice-president for Asia,
told a Harvard audience in a recent
speech.
In India, he pointed out, "popu-
lation is the major cau&e, &f:. de-
forestation and degradation of
water sheds. Recent remote sens-
ing of India's forest cover places it
at 11 per cent of India's land area,
a perilously low proportion given
the value of the forest in su.taining
the lives of the poor."
He said that global problems .uch
as acid rain, damage to the ozone
layer and global warming have
sparked debates between indus-
trial and developing countries
'about who is to blame and who
should pay.' He observed that
these debates underscore their
common concern and point to the
need for a joint approach that will
require additional financial support
from the industrial countries for
environmental programmes in the
develQli>ing countries.
TUmfflg to the environmentel
challenges facing Asia, Mr.
Karaosmanoglu said that these pro-
blems snouJd be seen in the con-
text of the- region's 2.5 billion
popul~tion, "constituting about 64
per cent of the total population of
all developing countries squeezed
on to 26 per cent of the land." In
order to survive, 'Asia's poor people
"are depleting the forests, soils,
and watersheds in their desperate
search for cultivable land, pastures,
building materials and fuelwood."
He also highlighted the negative
environmental consequences of the
region's rapid industrial growth.
The World Bank has provided
substantial funding for population
programmes in Asia, the World
Bank Vice-president noted, ex-
pressing confidence that govern-
ments in the region, especially in
the low income countries, "will
raise the priority of
planning as a developmental,
environmental, objective."
|
|
7 Page 7 |
▲back to top |
The Catholic Church "has now
become tho world's most active
proponent of natural family plann-
ing (N.F.P.), a morc effective
version of the old unreliable rhythm
method," and has been particlJ~arl.,
aggressive in promoting it in the
Third World, reports rime magazine.
A 1976 study by the World Health
Organization concluded that it pre-
vents conception as effectively as
artificial means. Called the ovula-
tion or Billings methods, it enables
a woman to determine her fertile
period by monitoring her cervical
mucus. Sister Cecilia, who runs
18 N.F.P. centres in Brazil, says it
is the ideal method for the poor
and illiterate because it "doesn't
cost anything, and the women
don't have to read or write to
figure out which are their fertile
days." Unlike the artificial methods,
however, N.F.P. requires a period
of training, usually about four
months. The method's other princi-
pal disadvantage is the monthly
requirement of voluntary absti-
nence during the woman's fertile
period, which may not elicit the
cooperation of macho males. A
catholic lay worker in Brazil says
the natural methods "are more
suitable for the middle or upper
classes, where the husband and
wife can discuss family planning.
Lifo in the slums is a whole diffe-
rent reality."
(World Deveiopment Forum,
Vol. 6, No. 19, 1988)
Small Family Norm in
Bangladesh
Attitudinal constraints to family
planning in Bangladesh are dis-
appearing at the local level with
the help of a recent series of
projects promoting "the small
family norm,"
Its main objective is to make
young men aware of Bangladesh's
population problem by inviting them
into fellow villagers' homes and
discussing family planning in a
casual atmosphere. These villagers,
"model families" consisting of two
parents and two children, explain
how they have used and benefited
from family planning, and then
encourage the young men to do
the same. Designated family
planning workers also attend the
meetings' to speak, to answer
questions, and to dispel m1sunder-
standings about family p'anning
within the context of Is!am.
Ambiguity over the way Islam
views family planning has often
been a major obstacle to increased
contraceptive use. These informal
group sessions help to establish
the acceptability of family planning
within the Islamic value system
as well as correct misinformation
about contraception.
(Pathways, Spring 1988)
World Bank Agenda to
Reduce Global Poverty
In the opinion of World Bank
President Barber B. Conable,
"Poverty on today's scale prevents
a billion people from having even
minimally acceptable standards of
living. To allow every fifth human
being on our planet to suffer su'Ch
an existence is a moral outrage.
It is more, it is bad economics, a
terrible waste of precious develop-
ment resources."
He has listed five major fronts
on which the World Bank intends
to focus attention:
1. securing eConomic growth;
2. combating hunger;
3. curbing excessive population
growth;
4. investing in education; and
5. protecting the interests of the
poor during periods of econo-
mic adjustment.
Mr. Conable says, "I realize that
population policy touches upon
sensitive cultural and religious
values, but the societies in which
population is growing rapidly must
accept that many perhaps most of
these new lives, will be mise·able,
malnourished and brief."
Recommendations
(Continued trom page 3)
programme in the states and areas
where it has not gained sufficient
momentum adopting area specific
strategies; mobilising political will
at all levels; reshaping of th<.
communication strategy for better
integrated health and family wel-
fare programme activities to be
planned and implemented in a
professional manner; setting up of
a sound management information
system; designing of comprehen-
sive tratning programmes for medi-
cal,··pat'8~medical and non-medi-
cal personnel; expanding the
number, scope and outreach of
voluntary organisations; r.edefin-
ing the role-of incentives and dis-
incentives on area to area basis;
implementing mass education and
health education programmes
effectively; giving preference to
family planning acceptors in all
the Government programmes and
schemes; taking steps to raise the
age of marriage; evolving a package
of family planning and MCH
services, beginning with ante-natal
care through to total family welfare
services; emphasi.,zing female lite-
racy on time-bound frame basis;
countering deep-rooted belief
supporting son preference; utilis-
ing Indian system of medicine and
homeopathy; generating a climate
of stronger motivation by involving
the local bodies, panchayats, and
village health guides and other
community leaders and workers
along with steps to improve the
management, quality of services
and monitoring and evaluation of
the family welfare programmes.
|
|
8 Page 8 |
▲back to top |
urbanisation and the steadily grow-
i ng threat to the fragile balance of
envi ronment, orderly management
of migration, generating full em-
ployment and absorbing the shock
of social change as well as con-
flicts engendered by cultural factors
or economic causes.
The true purpose and aim of
population policy having been now
recognised as the enhancement of
quality of life for all segments
constituting a society, the crux of
the problem was taking a fresh
look at population policies in a
wider perspective, with due atten-
tion to the human dimension,
Mr. Khanna emphasised.
iEtlh~cs <86"1lrdl IHiUlmalnl
VahJ!6S i~ IFamiUy
1P~8ii1ln~:ng
Recent breakthroughs in the field
of reproductive medicine have caus-
ed heated controversies world-
wide on the moral, social and legal
implications of fertility regulation.
In the last two decades, scientific
advances have made dramatic new
infertility treatments, contraceptive
methods and genetic engineering
techniques a reality. But in doing
so, they have posed new and
fundamental problems for health
workers and policy makers, legis-
lators and religious leaders in
every country.
In June 1988, the Geneva-based
Council for International Organiza-
tion of Medical Sciences (CIOMS)
organised the first international
conference to discuss the ethical
issues raised by recent technologi-
cal developments in family plann-
ing. Entitled 'Ethics and Human
Values in Family Planning', it was
held in Bangkok, Thailand and
attended by more than 150 health
care professionals, soc~al and bio'-
medical scientists, politicians,
lawyers, ethicists and clerics.
Various UN agencies and inter-
national organizations were asso-
ciated with the conference.
Delegates often expressed widely
differing views on the key themes
of the conference, including family
planning policies and programmes,
abortion, the acceptability of diffe-
rent contraceptive methods, inferti-
lity issu,essuch as in vitro fertiliza-
tion, embryo transfer and surrogate
motherhood, and research using
human subjects and genetic mate-
rial.
The conference did not attempt
to make recommendations on ethi-
cal questions in family planning,
but aimed to define and clarify the
issues and the areas of consensus.
The WHO desoribed the long-
term aim of the conference as 'to
help countries to adopt policies on
fertility regulation and to find the
best ways of introducing family
planning services without running
up against local sensitivities and
traditions',
CIO"MS is preparing reports
on the proceedings f.or publi-
cation, in' the hope that this
will 'stimulate continued dialogue
about these complex issues and
encourage' tolerance of different
views among different cultures:
"Family Planning Programmes
must not confine themselves to
family planning and family
health alone. They must reach
out to influence villagers to
think in terms of inter-relation-
ships between population,
health, the environment and
the sustainability of the
balance between people and
the natural systems on which
they depend."
- Mrs A vabai Wadia
IPPF President.
Published by the Family Planning Foundation, 198 Golf L.mks, New Delhi 1100O3. Te.I' 62.1.135' 6971583. 619278
Printed at the Statesman Press, The Statesman Ltd" Connaught Circus, New Delhl-11000 .